

Network Meta-analysis and Economic Evaluation of Neurostimulation Interventions for Chronic Nonsurgical Refractory Back Pain
- PMID: 38751011
- PMCID: PMC11309338
- DOI: 10.1097/AJP.0000000000001223
Network Meta-analysis and Economic Evaluation of Neurostimulation Interventions for Chronic Nonsurgical Refractory Back Pain
Abstract
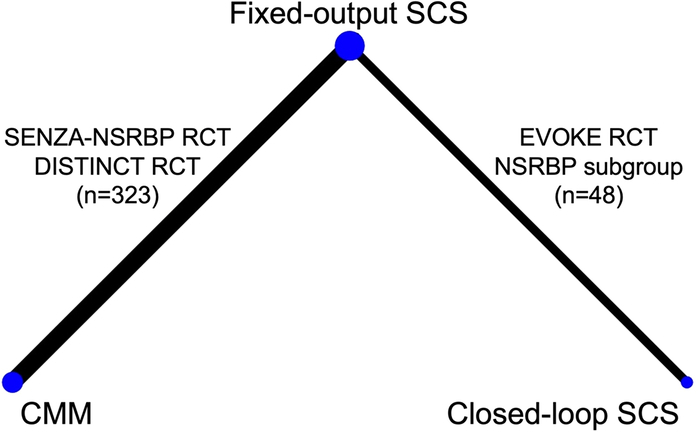
Objectives: Different types of spinal cord stimulation (SCS) have been evaluated for the management of chronic nonsurgical refractory back pain (NSRBP). A direct comparison between the different types of SCS or between closed-loop SCS with conventional medical management (CMM) for patients with NSRBP has not been previously conducted, and therefore, their relative effectiveness and cost-effectiveness remain unknown. The aim of this study was to perform a systematic review, network meta-analysis (NMA) and economic evaluation of closed-loop SCS compared with fixed-output SCS and CMM for patients with NSRBP.
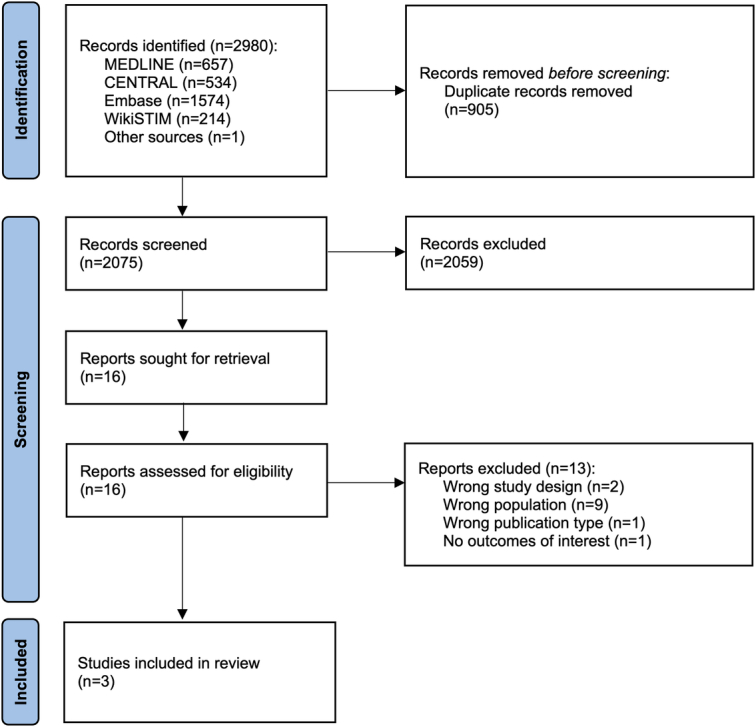
Methods: Databases were searched to September 8, 2023. Randomized controlled trials of SCS for NSRBP were included. The results of the studies were combined using fixed-effect NMA models. A cost-utility analysis was performed from the perspective of the UK National Health Service with results reported as incremental cost per quality-adjusted life-year (QALY).
Results: Closed-loop SCS resulted in statistically and clinically significant reductions in pain intensity (mean difference [MD] 32.72 [95% CrI 15.69-49.78]) and improvements in secondary outcomes (Oswestry Disability Index [ODI] and health-related quality of life [HRQoL]) compared with fixed-output SCS at 6-month follow-up. Compared with CMM, both closed-loop and fixed-output SCS resulted in statistically and clinically significant reductions in pain intensity (closed-loop SCS vs. CMM MD 101.58 [95% CrI 83.73-119.48]; fixed-output SCS versus CMM MD 68.86 [95% CrI 63.43-74.31]) and improvements in secondary outcomes (ODI and HRQoL). Cost-utility analysis showed that closed-loop SCS dominates fixed-output SCS and CMM, and fixed-output SCS also dominates CMM.
Discussion: Current evidence showed that closed-loop and fixed-output SCS provide more benefits and cost-savings compared with CMM for patients with NSRBP.
Copyright © 2024 The Author(s). Published by Wolters Kluwer Health, Inc.
Conflict of interest statement
This work was supported by Saluda Medical. S.E. reports consultancy fees from Medtronic, and Mainstay Medical outside the submitted work. He has received department research funding from the National Institute of Health Research, Saluda Medical and Medtronic. S.N. reports consultancy fees from Saluda Medical. A.B. MTech Access was commissioned by Saluda Medical to participate in this project. N.A.M. reports receiving grants from Neuros, Mesoblast, and Vivex Biologics, as well as consulting as a medical monitor for Saluda Medical, Nevro, Vivex Biologics, Mainstay, Sollis Therapeutics, and Vertos outside the submitted work. C.G. reports consulting fees and stock options received from Mainstay, personal fees from Mainstay, Saluda Medical, Persica, and Iliad outside the submitted work, research funded by Sollis, expert witness testimony fees, and serves as Editor-in-Chief of Pain Practice. B.B. reports an educational grant from Saluda Medical and consultancy fees from Salvia Bioelectronics, Medtronic and Abbott outside the submitted work. P.S.S. has received consultancy fees from Medtronic, Saluda Medical, Nalu, and Biotronic outside the submitted work, and has stock options from Saluda Medical and Nalu. M.M. reports no conflicts of interest. N.S., A.L., and R.V.D. are employees of Saluda Medical. R.V.D. has previously received consultancy fees from Mainstay Medical, Medtronic, and Saluda Medical outside the submitted work.
Figures
References
-
- Itz CJ, Geurts JW, van Kleef M, et al. . Clinical course of non-specific low back pain: a systematic review of prospective cohort studies set in primary care. Eur J Pain. 2013;17:5–15. - PubMed
-
- United States Bone and Joint Initiative . The burden of musculoskeletal diseases in the United States (BMUS). 2014. Accessed July 5, 2023. http://www.boneandjointburden.org
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
