

Quality of life outcomes after transobturator tape full removal surgeries: A monocentric experience
- PMID: 38751946
- PMCID: PMC11090767
- DOI: 10.1002/bco2.317
Quality of life outcomes after transobturator tape full removal surgeries: A monocentric experience
Erratum in
-
Erratum.BJUI Compass. 2024 Dec 30;5(12):1324-1329. doi: 10.1002/bco2.482. eCollection 2024 Dec. BJUI Compass. 2024. PMID: 39744071 Free PMC article.
Abstract
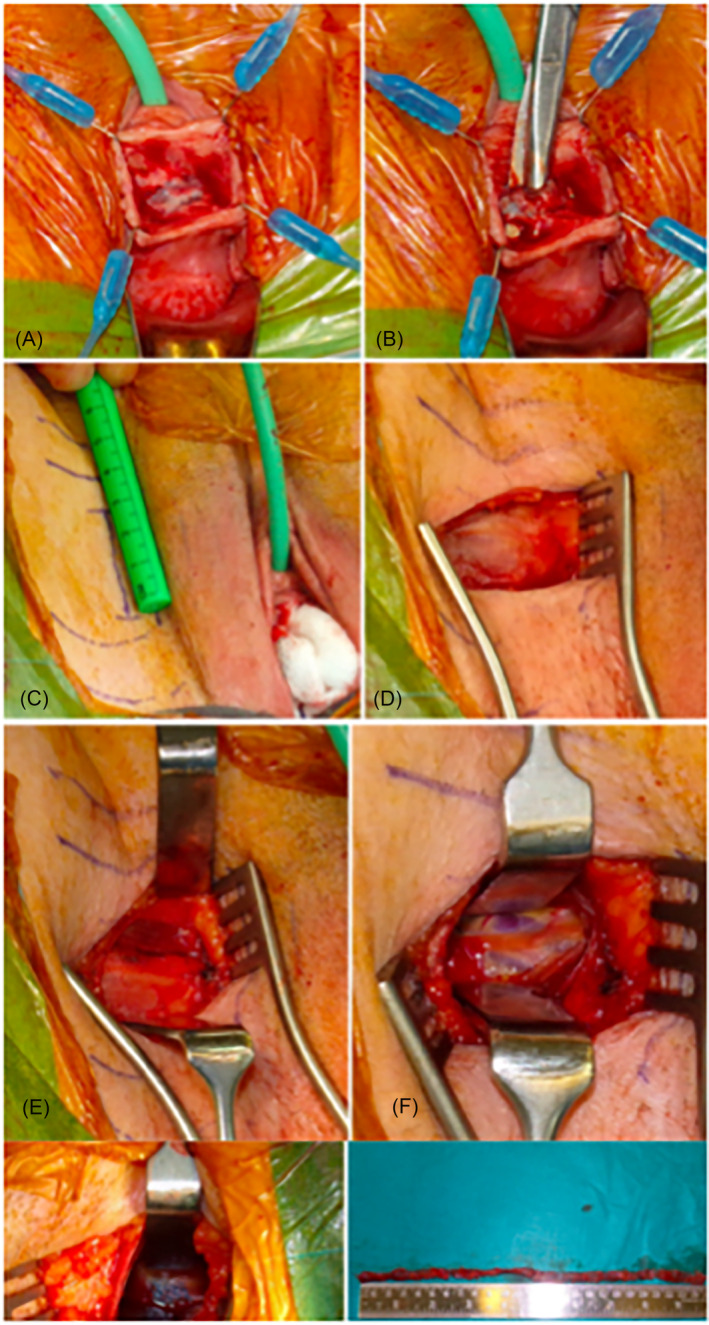
Objective: The objective of this study is to describe a standardised technique of full TOT removal with groin dissection and to report clinical improvement, satisfaction, safety and long-term functional, quality of life (QoL) and sexual QoL outcomes.
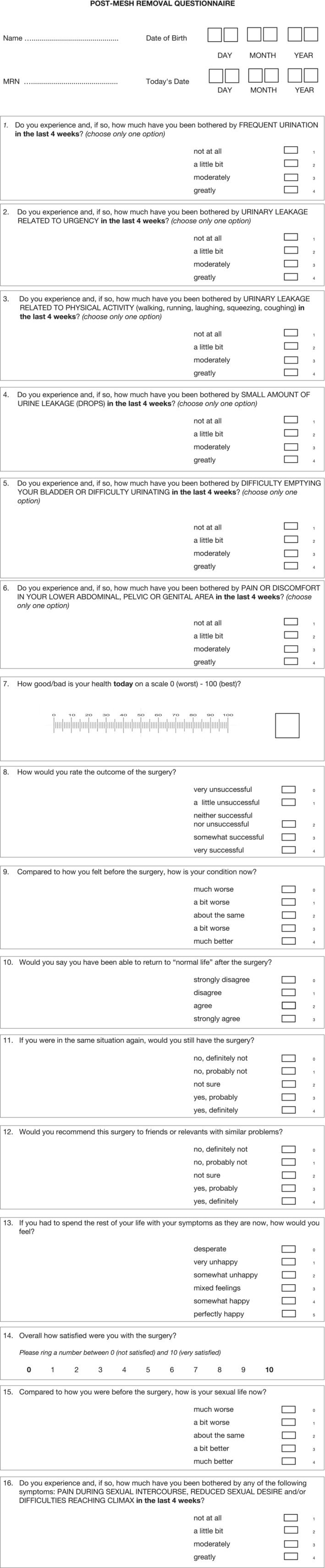
Materials and methods: A retrospective review enrolling all women who had full TOT removal, in a tertiary referral centre from May 2017 to November 2020. Functional outcomes, satisfaction and QoL were assessed using a bespoke composite questionnaire (UDI-6, EQ-5D-5L and ICIQ-S) with additional questions on sexual QoL. Secondary outcomes were post-operative recurrent stress urinary incontinence (SUI) and complication rate according to the Clavien-Dindo classification.
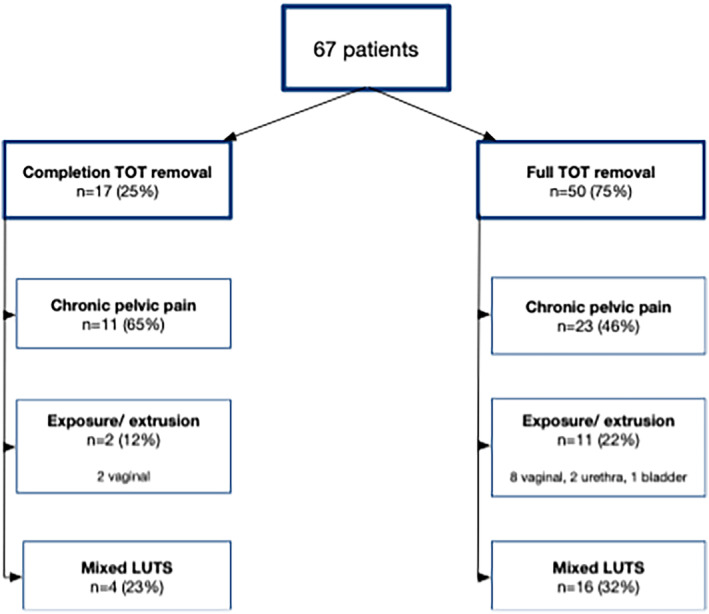
Results: Full TOT removal using a vaginal approach and bilateral groin/para-labial incisions was performed in 67 patients. Chronic pelvic pain was the main indication for mesh removal (51% of cases, n = 34). QoL questionnaires were answered by 43 patients. The satisfaction rate was high 86% (n = 37), and 81% (n = 35) of the patients considered the surgery successful. Seventy per cent (n = 30) of patients returned to having a sexual life after surgery. Recurrent SUI was reported in 32% (n = 14) of cases. The complication rate was 10% (7/67), all of them Clavien-Dindo ≤2.
Conclusion: Despite a high rate of postoperative bothersome SUI, full TOT removal with bilateral groin dissection improves pain and QoL. It is associated with a high overall satisfaction rate and an acceptable rate of complications.
Keywords: complications; mesh; quality of life; stress urinary incontinence; transobturator tape.
© 2024 The Authors. BJUI Compass published by John Wiley & Sons Ltd on behalf of BJU International Company.
Conflict of interest statement
The authors declare that they have NO affiliations with or involvement in any organisation or entity with any financial interest in the subject matter or materials discussed in this manuscript.
Figures
References
-
- MacCraith E, Cunnane EM, Joyce M, Forde JC, O'Brien FJ, Davis NF. Comparison of synthetic mesh erosion and chronic pain rates after surgery for pelvic organ prolapse and stress urinary incontinence: a systematic review. Int Urogynecology J. 2021;32(3):573–580. 10.1007/s00192-020-04612-x - DOI - PubMed
-
- Joint Writing Group of the American Urogynecologic Society and the International Urogynecological Association . Joint position statement on the management of mesh‐related complications for the FPMRS specialist. Female Pelvic Med Reconstr Surg. 2020;26(4):219–232. - PubMed
LinkOut - more resources
Full Text Sources