

Spondylodiscitis: A Diagnostic and Management Dilemma
- PMID: 38752024
- PMCID: PMC11094521
- DOI: 10.7759/cureus.58284
Spondylodiscitis: A Diagnostic and Management Dilemma
Abstract
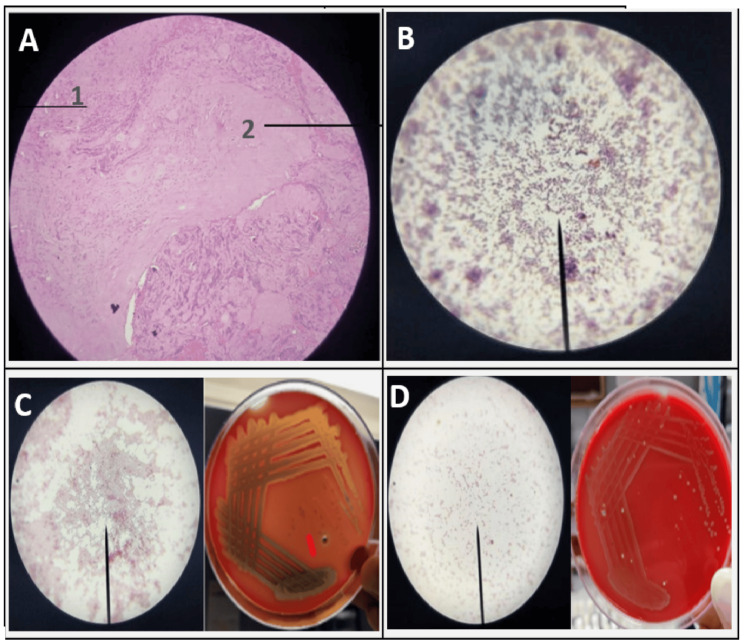
Aims Spondylodiscitis (SpD), a debilitating infective condition of the spine, mandates early diagnosis and institution of appropriate therapy, for which accurate microbiology and histological evaluation of the affected tissue is vital. The objectives of the study were to assess the correlation between clinical and magnetic resonance imaging (MRI) findings with histopathology (HPE) and microbiology (MB) in clinically diagnosed spondylodiscitis. Settings and design This was a prospective study of 34 consecutive patients reporting at the outpatient department of a tertiary hospital with clinical and imaging features of SpD, who underwent image-guided/surgical biopsy of lesions. Methods and material The provisional diagnosis of SpD in all patients was made on the combined basis of clinical profile and MRI Spine findings. Tissue samples in all patients, obtained by either open surgery or CT-guided biopsy, were subjected to HPE and MB analysis. Results SpD has a bimodal age distribution with the majority of patients being males in the fourth to fifth decades. Only raised erythrocyte sedimentation rate (ESR) was consistently seen amongst laboratory parameters, with leucocytosis being added pointer towards pyogenic etiology. MRI remained the imaging modality of choice for SpD but was not dependable for etiologic differentiation. On HPE and MB evaluations, 24 patients (71%) had findings consistent with infective SpD, while combined results augmented etiologic confirmation for 28 patients (82.4%). HPE was more sensitive than traditional MB methods to determine etiology in SpD, but the addition of the GeneXpert (Cepheid, Sunnyvale, California, United States) technique improved the MB positivity rate, especially in patients with tubercular SpD. Six patients (17.6%) with both negative HPE and MB results were categorized as 'Non-specific' SpD. Conclusions SpD poses a challenge to determine the etiology for the administration of specific antimicrobial therapy. A stratified standard institutional approach needs adoption to systematically evaluate SpD patients by having a high index of clinical suspicion, early imaging, followed by tissue biopsy for HPE and MB. Despite efforts to reach a diagnosis, a subset of patients without conclusive etiologic agent identification would remain as 'Non-specific', needing empiric antibiotic treatment based on clinico-radiologic profile.
Keywords: histopathology & microbiology; pott's disease; pyogenic; spine diseases; spondylodiscitis; tuberculous spondylitis.
Copyright © 2024, George et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Utility of magnetic resonance imaging in the differential diagnosis of tubercular and pyogenic spondylodiscitis. Galhotra RD, Jain T, Sandhu P, Galhotra V. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4518416/ J Nat Sci Biol Med. 2015;6:388–393. - PMC - PubMed
-
- Spontaneous spondylodiscitis - epidemiology, clinical features, diagnosis and treatment. Petkova AS, Zhelyazkov CB, Kitov BD. Folia Med (Plovdiv) 2017;59:254–260. - PubMed
-
- The MRI appearances of early vertebral osteomyelitis and discitis. Dunbar JA, Sandoe JA, Rao AS, Crimmins DW, Baig W, Rankine JJ. Clin Radiol. 2010;65:974–981. - PubMed
-
- The role of histology in the diagnosis of spondylodiscitis: correlation with clinical and microbiological findings. Iwata E, Scarborough M, Bowden G, McNally M, Tanaka Y, Athanasou NA. Bone Joint J. 2019;101-B:246–252. - PubMed
-
- Spondylodiscitis: update on diagnosis and management. Gouliouris T, Aliyu SH, Brown NM. J Antimicrob Chemother. 2010;65 Suppl 3:0–24. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous