

Evolving growth hormone deficiency: proof of concept
- PMID: 38752175
- PMCID: PMC11095394
- DOI: 10.3389/fendo.2024.1398171
Evolving growth hormone deficiency: proof of concept
Abstract
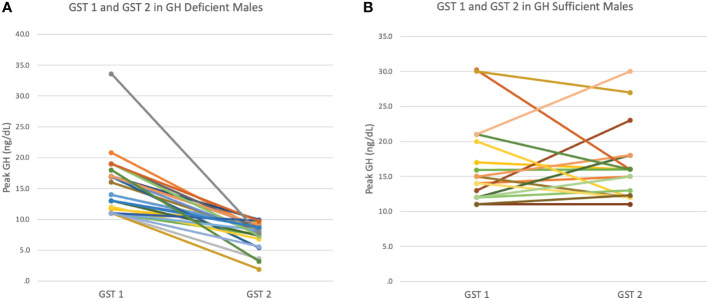
Introduction: We present the evolution of GHD in adolescent males with persistent growth failure, in whom the diagnosis was established after a second GH stimulation test (GST).
Methods: We performed a retrospective chart review of children who presented for short stature (height less < 2SD for mean/mid-parental height) and/or growth failure (sustained growth velocity < 0 SD) to pediatric endocrinology at Mount Sinai Kravis Children's Hospital, New York and who had 2 GSTs. Data collected from electronic medical records were analyzed using SPSS v28.0.
Results: Of 53 patients included, 42 were males. Average GH peak on initial GST was 15.48 ± 4.92 ng/ml, at 10.07 ± 2.65 years, mean height -1.68 ± 0.56SD(28% had <2SD), IGF-1 -1.00 ± 0.88SD. After 2.23 ± 1.22 years, at 12.04 ± 2.41years, height SDs decreased to -1.82 ± 0.63SD and IGF-1 was -1.08 ± 0.84SD. At repeat GST, average GH peak was 7.59 ± 2.12 ng/dL, with 36% ≤7 ng/dl and 32% in puberty. 12 males reached adult height of 0.08 ± 0.69 SD with a mean height gain of 1.83 ± 0.56SD(p<0.005), IGF-1 of -1.15 ± 0.81SD after 4.64 ± 1.4 years of GH.
Conclusion: We offer evidence for Evolving Growth Hormone Deficiency (EGHD) through repeat GST in children with persistent growth slowdown, even with pubertal progression; emphasizing the need for careful longitudinal follow-up to make accurate diagnosis.
Keywords: growth; growth hormone deficiency; growth hormone stimulation test; growth hormone therapy; idiopathic short stature.
Copyright © 2024 Chimatapu, Sethuram, Samuels, Klomhaus, Mintz, Savage and Rapaport.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Growth response to growth hormone (GH) treatment in children with GH deficiency (GHD) and those with idiopathic short stature (ISS) based on their pretreatment insulin-like growth factor 1 (IGFI) levels and at diagnosis and IGFI increment on treatment.J Pediatr Endocrinol Metab. 2021 Jul 22;34(10):1263-1271. doi: 10.1515/jpem-2021-0389. Print 2021 Oct 26. J Pediatr Endocrinol Metab. 2021. PMID: 34291621 Clinical Trial.
-
Responses to growth hormone (GH) therapy in short children with normal GH secretion and no bone age delay: an analysis of potential factors affecting their response to rhGH therapy. A controlled study.Acta Biomed. 2019 Sep 23;90(8-S):43-51. doi: 10.23750/abm.v90i8-S.8506. Acta Biomed. 2019. PMID: 31544806 Free PMC article.
-
[Efficacy and safety of recombinant human growth hormone solution in children with growth hormone deficiency in China: a multicenter trial].Zhonghua Er Ke Za Zhi. 2009 Jan;47(1):48-52. Zhonghua Er Ke Za Zhi. 2009. PMID: 19573383 Clinical Trial. Chinese.
-
Growth hormone responses during arginine and clonidine stimulation test: Correlations with patients' auxological and metabolic parameters in a single centre study.Growth Horm IGF Res. 2023 Feb;68:101522. doi: 10.1016/j.ghir.2022.101522. Epub 2022 Dec 5. Growth Horm IGF Res. 2023. PMID: 36502626 Review.
-
Magnetic resonance images of 91 children with different causes of short stature: pituitary size reflects growth hormone secretion.Eur J Pediatr. 1997 Oct;156(10):758-63. doi: 10.1007/s004310050707. Eur J Pediatr. 1997. PMID: 9365063 Review.
Cited by
-
Biomarkers of GH deficiency identified in untreated and GH-treated Pit-1 mutant mice.Front Endocrinol (Lausanne). 2025 Apr 30;16:1539797. doi: 10.3389/fendo.2025.1539797. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 40370773 Free PMC article.
References
-
- Collett-Solberg PF, Ambler G, Backeljauw PF, Bidlingmaier M, Biller BMK, Boguszewski MCS, et al. . Diagnosis, genetics, and therapy of short stature in children: A growth hormone research society international perspective. Horm Res Paediatr. (2019) 92:1–14. doi: 10.1159/000502231 - DOI - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous