

European Stroke Organisation and European Society for Minimally Invasive Neurological Therapy guideline on acute management of basilar artery occlusion
- PMID: 38752743
- PMCID: PMC11569583
- DOI: 10.1177/23969873241257223
European Stroke Organisation and European Society for Minimally Invasive Neurological Therapy guideline on acute management of basilar artery occlusion
Abstract
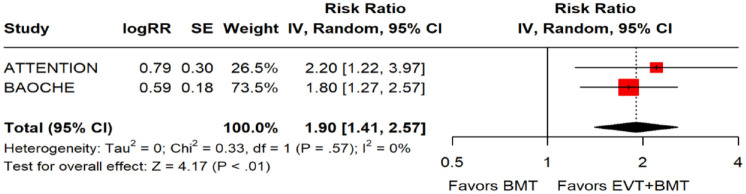
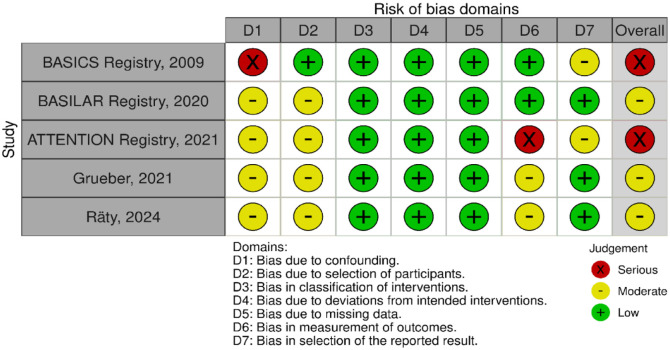
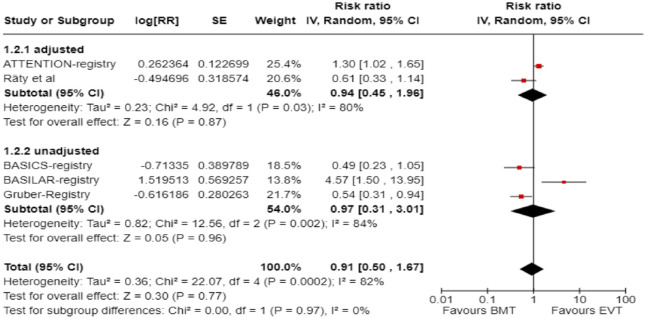
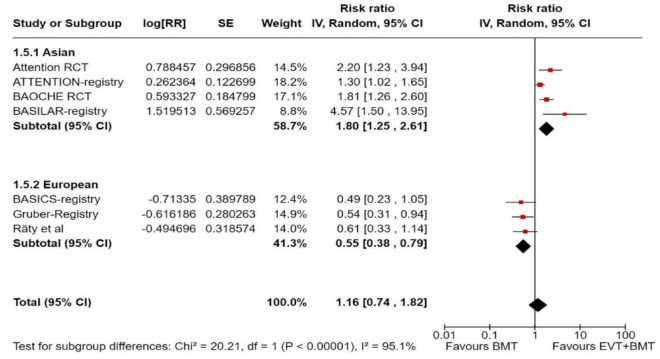
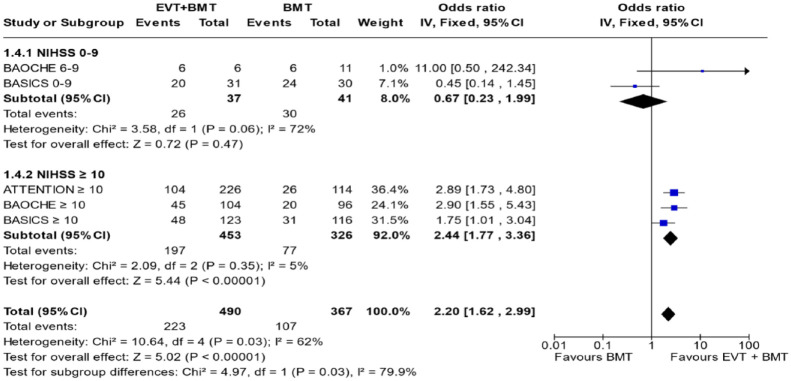
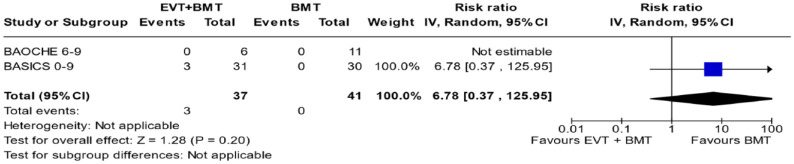
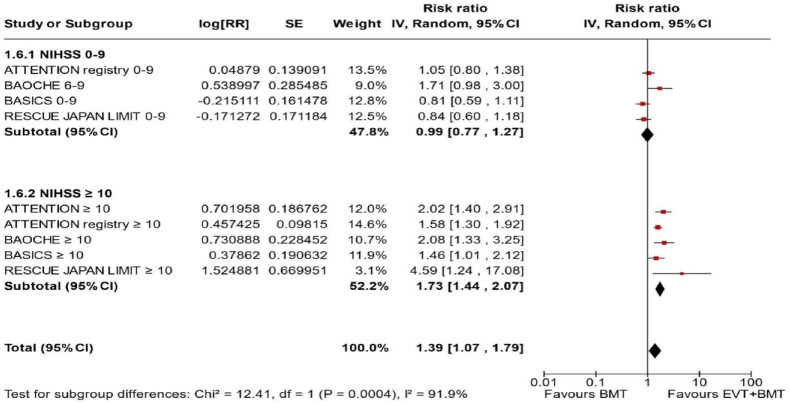
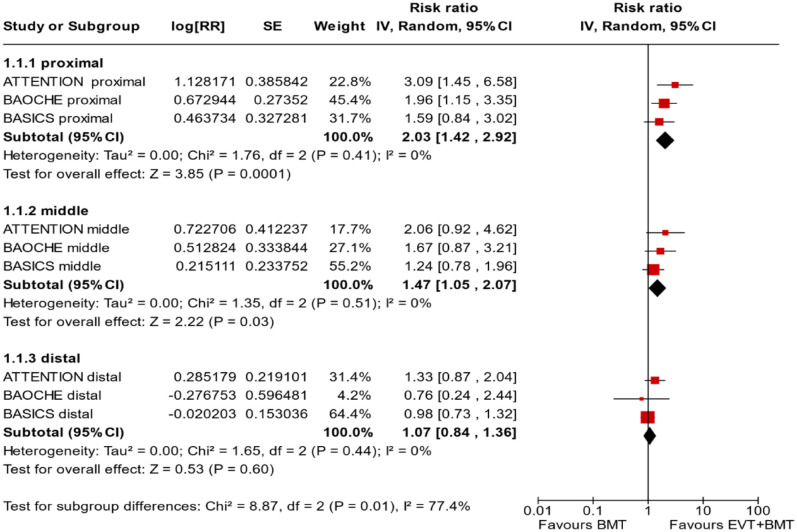
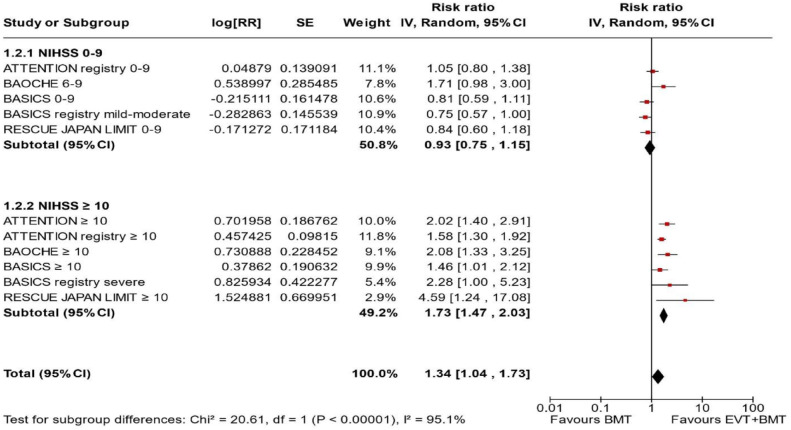
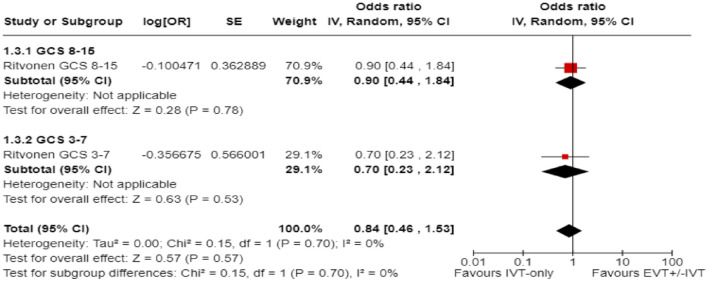
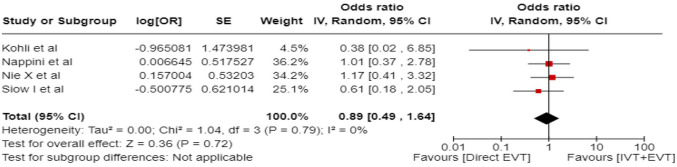
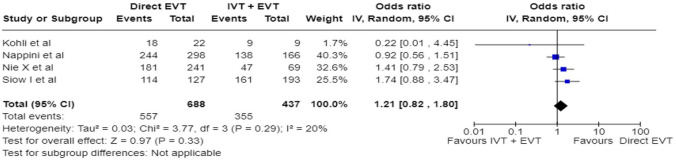
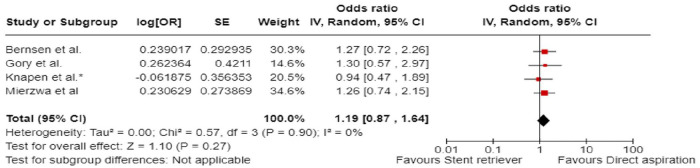
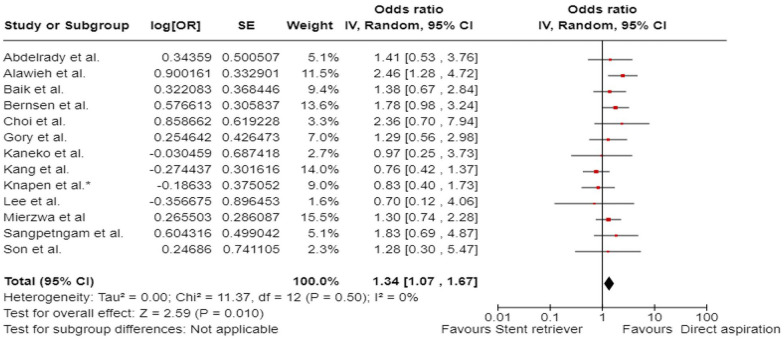
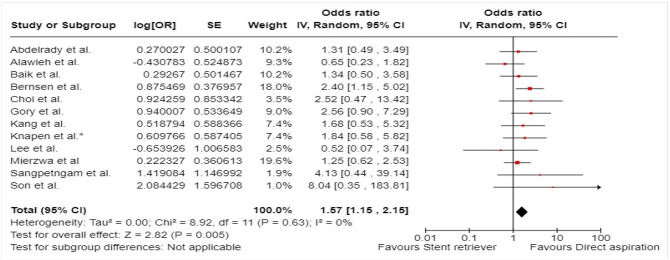
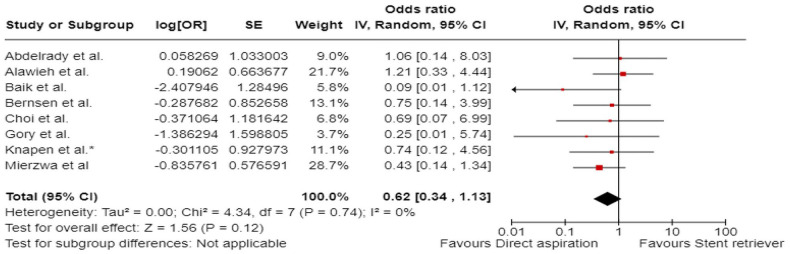
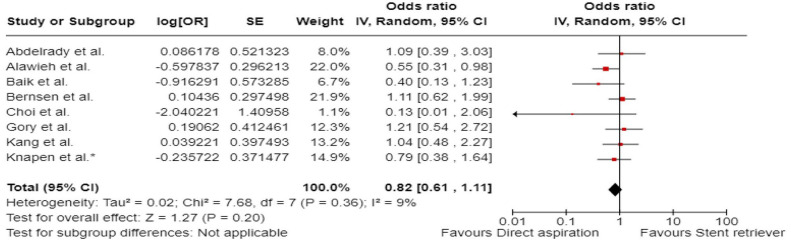
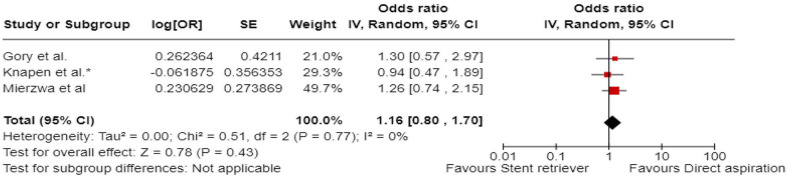
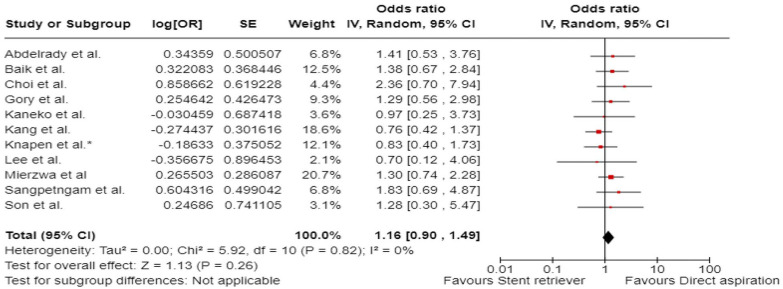
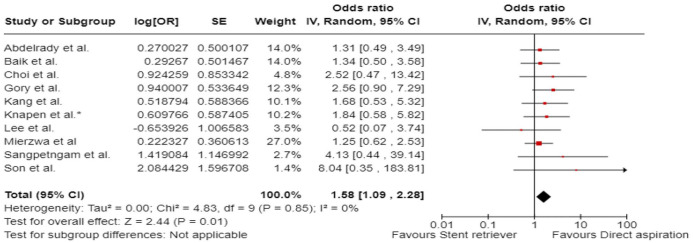
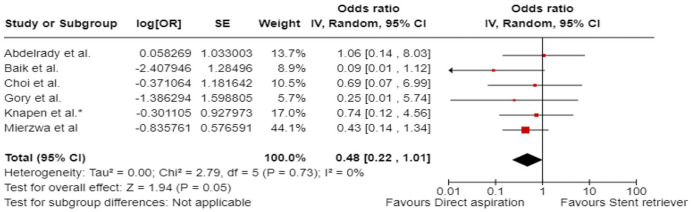
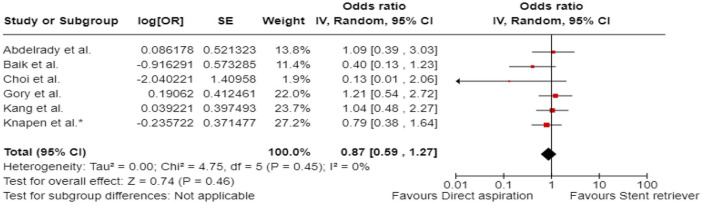
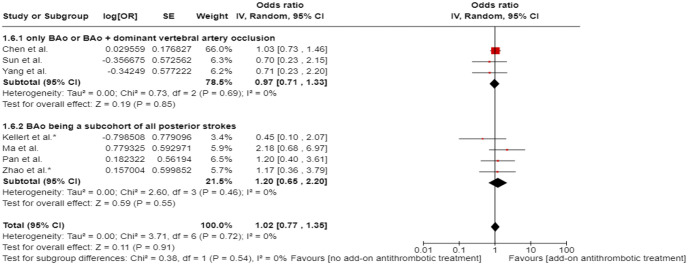
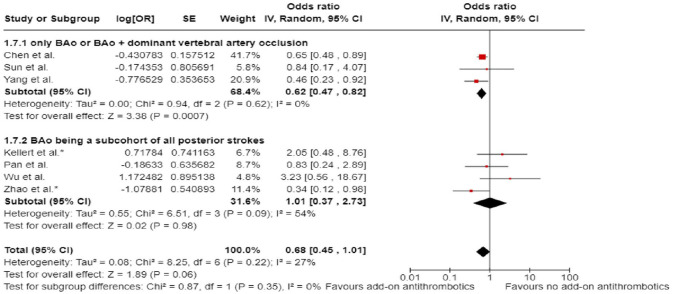
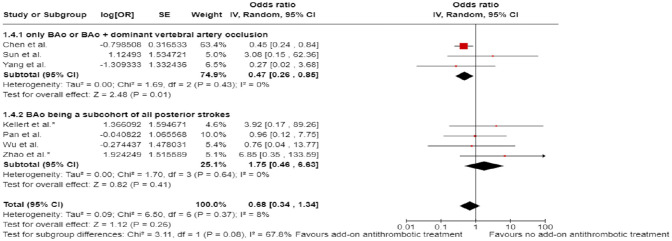
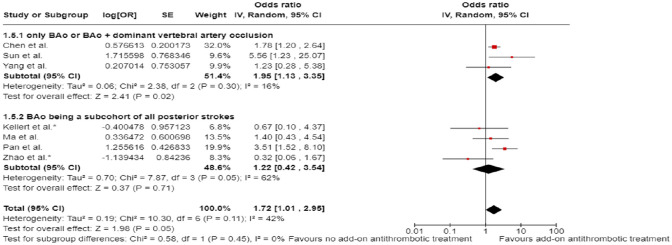
The aim of the present European Stroke Organisation (ESO) guideline is to provide evidence-based recommendations on the acute management of patients with basilar artery occlusion (BAO). These guidelines were prepared following the Standard Operational Procedure of the ESO and according to the GRADE methodology. Although BAO accounts for only 1%-2% of all strokes, it has very poor natural outcome. We identified 10 relevant clinical situations and formulated the corresponding Population Intervention Comparator Outcomes (PICO) questions, based on which a systematic literature search and review was performed. The working group consisted of 10 voting members (five representing ESO and five ESMINT) and three non-voting junior members. The certainty of evidence was generally very low. In many PICOs, available data were scarce or lacking, hence, we provided expert consensus statements. First, we compared intravenous thrombolysis (IVT) to no IVT, but specific BAO-related data do not exist. Yet, historically, IVT was standard of care for BAO patients who were also included (albeit in small numbers) in IVT trials. Non-randomised studies of IVT-only cohorts showed high proportion of favourable outcomes. Expert Consensus suggests using IVT up to 24 h unless otherwise contraindicated. We further suggest IVT plus endovascular treatment (EVT) over direct EVT. EVT on top of best medical treatment (BMT) was compared to BMT alone within 6 and 6-24 h from last seen well. In both time windows, we observed a different effect of treatment depending on (a) the region where the patients were treated (Europe vs. Asia), (b) on the proportion of IVT in the BMT arm, and (c) on the initial stroke severity. In case of high proportion of IVT in the BMT group and in patients with NIHSS below 10, EVT plus BMT was not found better than BMT alone. Based on very low certainty of evidence, we suggest EVT + BMT over BMT alone (i.e. based on results of patients with at least 10 NIHSS points and a low proportion of IVT in BMT). For patients with an NIHSS below 10, we found no evidence to recommend EVT over BMT. In fact, BMT was non-significantly better and safer than EVT. Furthermore, we found a stronger treatment effect of EVT + BMT over BMT alone in proximal and middle locations of BAO compared to distal location. While recommendations for patients without extensive early ischaemic changes in the posterior fossa can, in general, follow those of other PICOs, we formulated an Expert Consensus Statement suggesting against reperfusion therapy in those with extensive bilateral and/or brainstem ischaemic changes. Another Expert Consensus suggests reperfusion therapy regardless of collateral scores. Based on limited evidence, we suggest direct aspiration over stent retriever as the first-line strategy of mechanical thrombectomy. As an Expert Consensus, we suggest rescue percutaneous transluminal angioplasty and/or stenting after a failed EVT procedure. Finally, based on very low certainty of evidence, we suggest add-on antithrombotic treatment during EVT or within 24 h after EVT in patients with no concomitant IVT and in whom EVT was complicated (defined as failed or imminent re-occlusion, or need for additional stenting or angioplasty).
Keywords: Guideline; acute management; basilar artery occlusion; endovascular treatment; posterior circulation; stroke; systematic review; thrombolysis.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: All authors have completed a declaration of competing interests and details are available in Supplemental Table 1.
Figures






Similar articles
-
Reperfusion treatment in basilar artery occlusion presenting with mild symptoms.Eur Stroke J. 2025 Mar;10(1):46-55. doi: 10.1177/23969873241272517. Epub 2024 Aug 20. Eur Stroke J. 2025. PMID: 39162131 Free PMC article.
-
European Stroke Organisation (ESO) and European Society for Minimally Invasive Neurological Therapy (ESMINT) guideline on acute management of basilar artery occlusion.J Neurointerv Surg. 2024 Aug 14;16(9):e7. doi: 10.1136/jnis-2024-022053. J Neurointerv Surg. 2024. PMID: 39043395 Free PMC article.
-
IV Thrombolysis in Basilar Artery Occlusion: Outcomes and Comparison With Endovascular Thrombectomy.Neurology. 2024 Apr 23;102(8):e209249. doi: 10.1212/WNL.0000000000209249. Epub 2024 Mar 26. Neurology. 2024. PMID: 38531004
-
Focused update to guidelines for endovascular therapy for emergent large vessel occlusion: basilar artery occlusion patients.J Neurointerv Surg. 2024 Jul 16;16(8):752-755. doi: 10.1136/jnis-2024-021705. J Neurointerv Surg. 2024. PMID: 38670791 Review.
-
Efficacy and safety of thrombectomy with or without intravenous thrombolysis in the treatment of acute basilar artery occlusion ischemic stroke: an updated systematic review and meta-analysis.Front Neurol. 2024 Oct 24;15:1433158. doi: 10.3389/fneur.2024.1433158. eCollection 2024. Front Neurol. 2024. PMID: 39512275 Free PMC article.
Cited by
-
Thrombectomy Alone or Alongside Intravenous Thrombolysis in Managing Acute Ischemic Stroke Caused by Basilar Artery Occlusion: A Multicenter Observational Study.AJNR Am J Neuroradiol. 2025 Apr 2;46(4):706-711. doi: 10.3174/ajnr.A8520. AJNR Am J Neuroradiol. 2025. PMID: 39349308
-
Reperfusion treatment in basilar artery occlusion presenting with mild symptoms.Eur Stroke J. 2025 Mar;10(1):46-55. doi: 10.1177/23969873241272517. Epub 2024 Aug 20. Eur Stroke J. 2025. PMID: 39162131 Free PMC article.
-
Intravenous thrombolysis before endovascular treatment in acute vertebrobasilar occlusions: Pooled analysis of the French and German Stroke Registries.Eur Stroke J. 2025 Apr 16:23969873251333652. doi: 10.1177/23969873251333652. Online ahead of print. Eur Stroke J. 2025. PMID: 40237587 Free PMC article.
-
Comparison of Aspiration and Stent Retriever in Acute Basilar Artery Occlusion: A Subanalysis of the K-NET Registry.J Neuroendovasc Ther. 2025;19(1):2025-0067. doi: 10.5797/jnet.oa.2025-0067. Epub 2025 Aug 15. J Neuroendovasc Ther. 2025. PMID: 40827256 Free PMC article.
-
Endovascular Treatment for Basilar Artery Occlusion.J Clin Med. 2024 Jul 16;13(14):4153. doi: 10.3390/jcm13144153. J Clin Med. 2024. PMID: 39064193 Free PMC article. Review.
References
-
- Joundi RA, Sun JL, Xian Y, et al.. Association between endovascular therapy time to treatment and outcomes in patients with basilar artery occlusion. Circulation 2022; 145: 896–905. - PubMed
-
- Schonewille WJ, Wijman CAC, Michel P, et al.. Treatment and outcomes of acute basilar artery occlusion in the Basilar Artery International Cooperation Study (BASICS): a prospective registry study. Lancet Neurol 2009; 8: 724–730. - PubMed
-
- Goyal M, Menon BK, van Zwam WH, et al.. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet 2016; 387: 1723–1731. - PubMed
-
- Turc G, Bhogal P, Fischer U, et al.. European Stroke Organisation (ESO) – European Society for Minimally Invasive Neurological Therapy (ESMINT) guidelines on mechanical thrombectomy in acute ischemic stroke. J Neurointerv Surg 2023; 15: e8. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
