

European Stroke Organisation (ESO) Guidelines on the diagnosis and management of patent foramen ovale (PFO) after stroke
- PMID: 38752755
- PMCID: PMC11569559
- DOI: 10.1177/23969873241247978
European Stroke Organisation (ESO) Guidelines on the diagnosis and management of patent foramen ovale (PFO) after stroke
Abstract
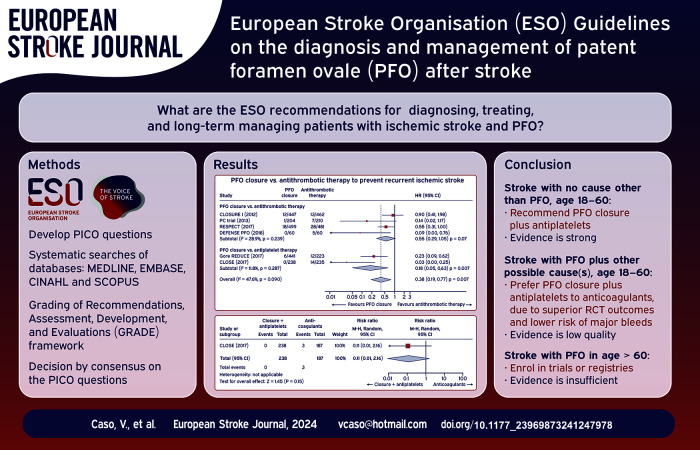
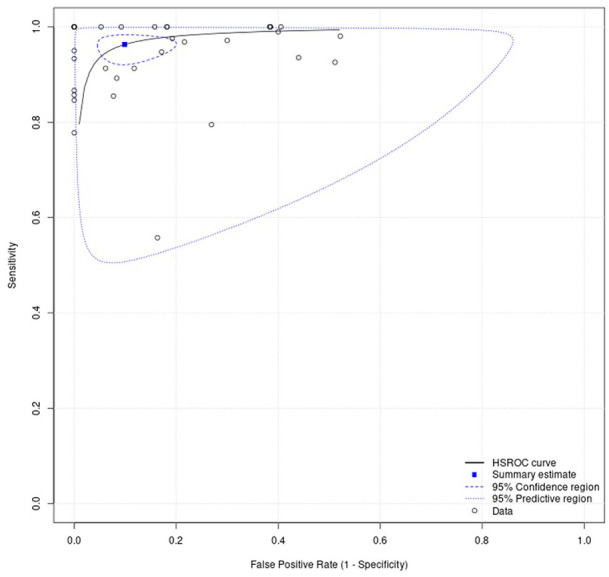
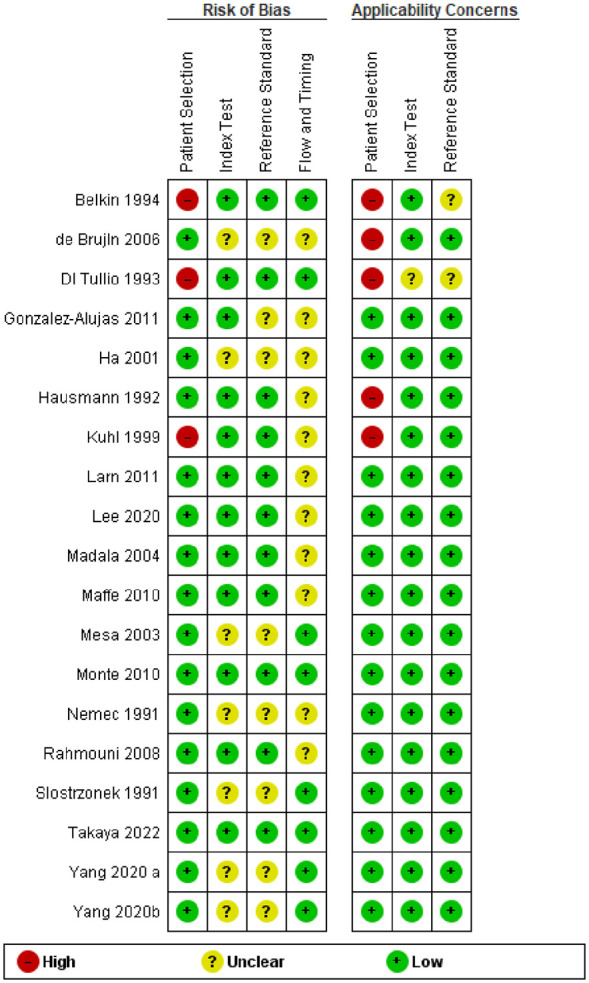
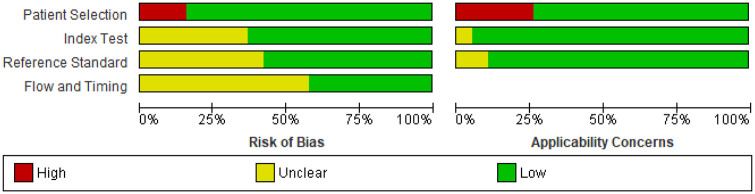
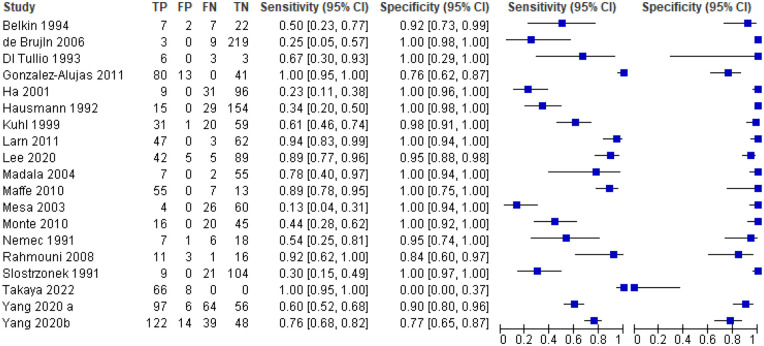
Patent foramen ovale (PFO) is frequently identified in young patients with cryptogenic ischaemic stroke. Potential stroke mechanisms include paradoxical embolism from a venous clot which traverses the PFO, in situ clot formation within the PFO, and atrial arrhythmias due to electrical signalling disruption. The purpose of this guideline is to provide recommendations for diagnosing, treating, and long-term managing patients with ischaemic stroke and PFO. Conversely, Transient Ischaemic Attack (TIA) was not considered an index event in this context because only one RCT involved TIA patients. However, this subgroup analysis showed no significant differences between TIA and stroke outcomes. The working group identified questions and outcomes, graded evidence, and developed recommendations following the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) approach and the European Stroke Organisation (ESO) standard operating procedure for guideline development. This document underwent peer-review by independent experts and members of the ESO Guideline Board and Executive Committee. The working group acknowledges the current evidentiary gap in delineating an unequivocal diagnostic algorithm for the detection of PFO. Although transoesophageal echocardiography is conventionally held as the most accurate diagnostic tool for PFO identification, its status as the 'gold standard' remains unsubstantiated by rigorously validated evidence. We found high-quality evidence to recommend PFO closure plus antiplatelet therapy in selected patients aged 18-60 years in whom no other evident cause of stroke is found but a PFO (i.e. PFO-associated stroke). The PASCAL classification system can be used to select such candidates for PFO closure. Patients with both a large right-to-left shunt and an atrial septal aneurysm benefit most from PFO closure. There is insufficient evidence to make an evidence-based recommendation on PFO closure in patients older than 60 and younger than 18 years. We found low quality evidence to suggest against PFO closure in patients with unlikely PFO-related stroke according to the PASCAL classification, except in specific scenarios (Expert Consensus). We suggest against long-term anticoagulation in patients with PFO-associated stroke unless anticoagulation is indicated for other medical reasons. Regarding the long-term AF monitoring after PFO closure, the working group concluded that there remains significant uncertainty regarding the risks and benefits associated with the use of long-term cardiac monitoring, such as implantable loop recorders. This document provides additional guidance, in the form of evidence-based recommendations or expert consensus statements, on diagnostic methods for PFO detection, and medical management after PFO closure.
Keywords: PFO closure; Patent foramen ovale; anticoagulation; antiplatelets; atrial fibrillation; stroke.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures









References
-
- Saver JL. Cryptogenic stroke. New Engl J Med 2016; 375: e26. - PubMed
-
- Saver JL, Mattle HP, Thaler D. Patent foramen ovale closure versus medical therapy for cryptogenic ischemic stroke: a topical review. Stroke 2018; 49: 1541–1548. - PubMed
-
- Pristipino C, Sievert H, D'Ascenzo F, et al. European position paper on the management of patients with patent foramen ovale. General approach and left circulation thromboembolism. Eur Heart J 2019; 40: 3182–3195. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
