

Clustering Identifies Subtypes With Different Phenotypic Characteristics in Women With Polycystic Ovary Syndrome
- PMID: 38753423
- PMCID: PMC11570376
- DOI: 10.1210/clinem/dgae298
Clustering Identifies Subtypes With Different Phenotypic Characteristics in Women With Polycystic Ovary Syndrome
Abstract
Context: Hierarchical clustering (HC) identifies subtypes of polycystic ovary syndrome (PCOS).
Objective: This work aimed to identify clinically significant subtypes in a PCOS cohort diagnosed with the Rotterdam criteria and to further characterize the distinct subtypes.
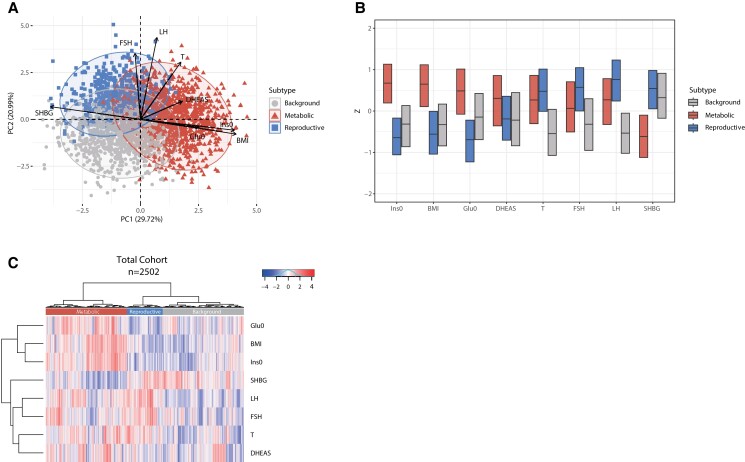
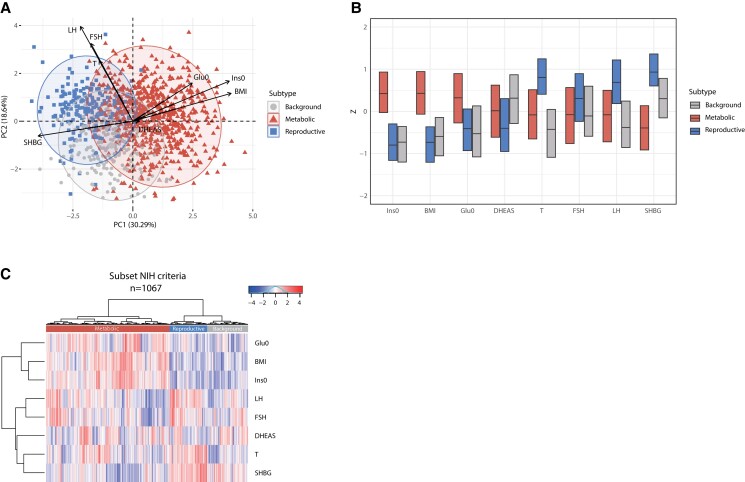
Methods: Clustering was performed using the variables body mass index (BMI), luteinizing hormone (LH), follicle-stimulating hormone, dehydroepiandrosterone sulfate, sex hormone-binding globulin (SHBG), testosterone, insulin, and glucose. Subtype characterization was performed by analyzing the variables estradiol, androstenedione, dehydroepiandrosterone, cortisol, anti-Müllerian hormone (AMH), total follicle count (TFC), lipid profile, and blood pressure. Study participants were girls and women who attended our university hospital for reproductive endocrinology screening between February 1993 and February 2021. In total, 2502 female participants of European ancestry, aged 13 to 45 years with PCOS (according to the Rotterdam criteria), were included. A subset of these (n = 1067) fulfilled the National Institutes of Health criteria (ovulatory dysfunction and hyperandrogenism). Main outcome measures included the identification of distinct PCOS subtypes using cluster analysis. Additional clinical variables associated with these subtypes were assessed.
Results: Metabolic, reproductive, and background PCOS subtypes were identified. In addition to high LH and SHBG levels, the reproductive subtype had the highest TFC and levels of AMH (all P < .001). In addition to high BMI and insulin levels, the metabolic subtype had higher low-density lipoprotein levels and higher systolic and diastolic blood pressure (all P < .001). The background subtype had lower androstenedione levels and features of the other 2 subtypes.
Conclusion: Reproductive and metabolic traits not used for subtyping differed significantly in the subtypes. These findings suggest that the subtypes capture distinct PCOS causal pathways.
Keywords: PCOS; cluster analysis; metabolic; reproductive; subtypes.
© The Author(s) 2024. Published by Oxford University Press on behalf of the Endocrine Society.
Figures
References
-
- Bozdag G, Mumusoglu S, Zengin D, Karabulut E, Yildiz BO. The prevalence and phenotypic features of polycystic ovary syndrome: a systematic review and meta-analysis. Hum Reprod. 2016;31(12):2841‐2855. - PubMed
-
- Lizneva D, Suturina L, Walker W, Brakta S, Gavrilova-Jordan L, Azziz R. Criteria, prevalence, and phenotypes of polycystic ovary syndrome. Fertil Steril. 2016;106(1):6‐15. - PubMed
-
- Neven ACH, Laven J, Teede HJ, Boyle JA. A summary on polycystic ovary syndrome: diagnostic criteria, prevalence, clinical manifestations, and management according to the latest international guidelines. Semin Reprod Med. 2018;36(1):5‐12. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
