

Unveiling the proteome-wide autoreactome enables enhanced evaluation of emerging CAR T cell therapies in autoimmunity
- PMID: 38753445
- PMCID: PMC11213466
- DOI: 10.1172/JCI180012
Unveiling the proteome-wide autoreactome enables enhanced evaluation of emerging CAR T cell therapies in autoimmunity
Abstract
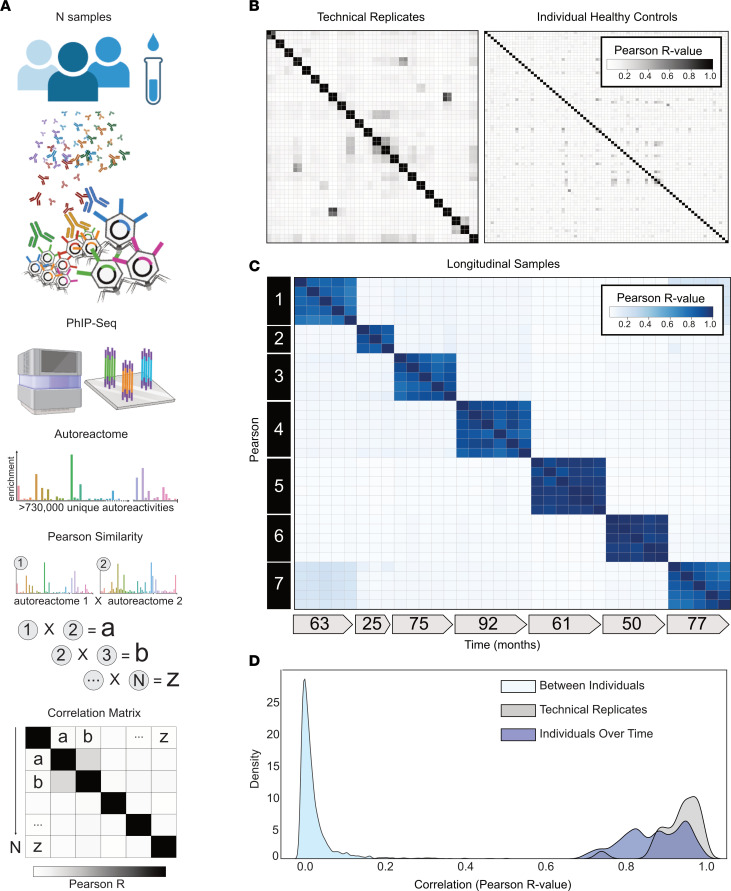
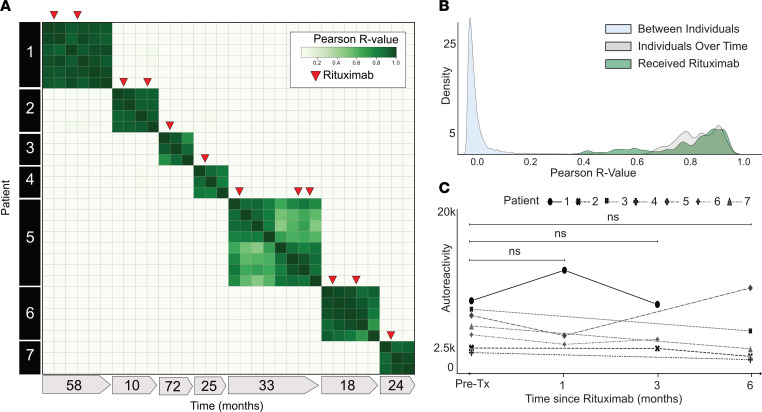
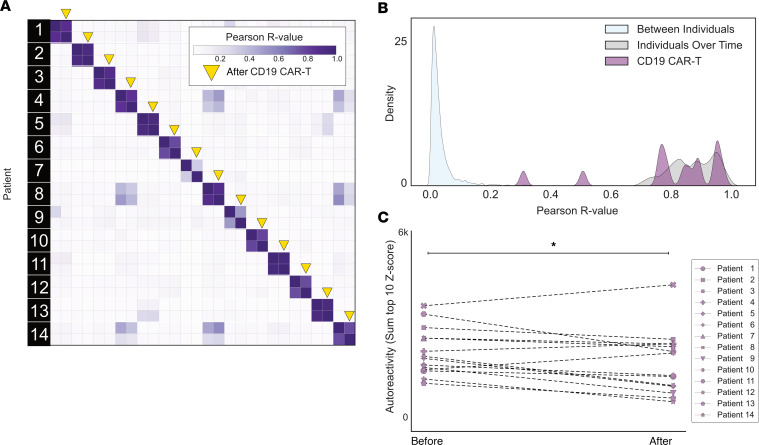
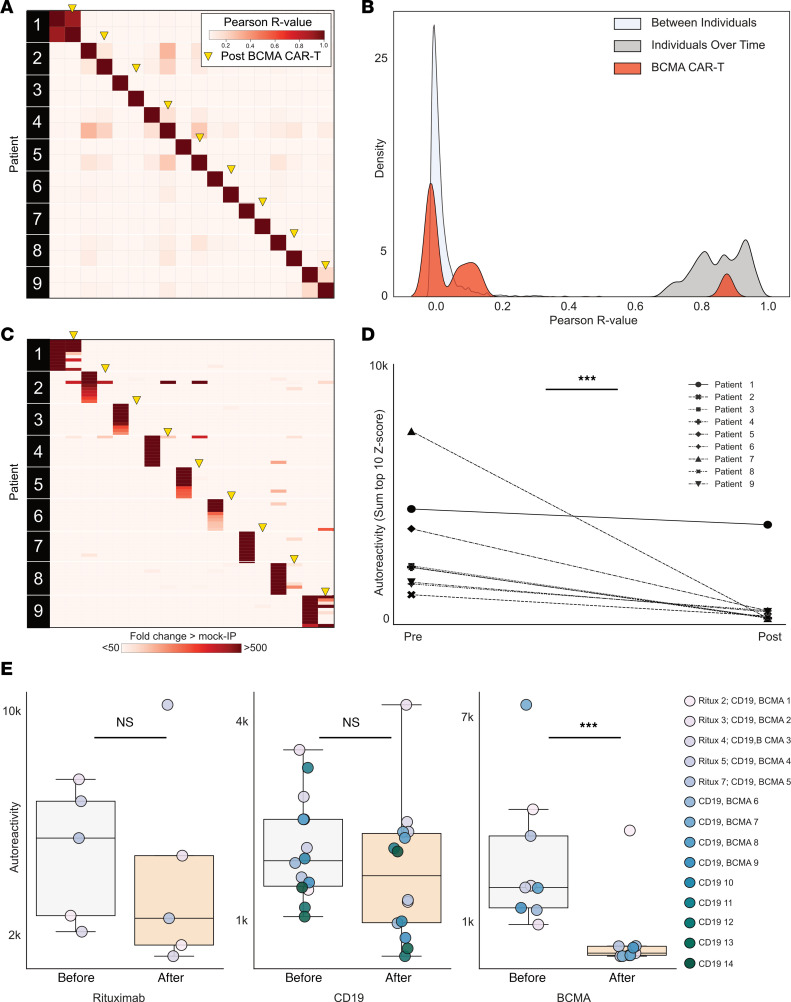
Given the global surge in autoimmune diseases, it is critical to evaluate emerging therapeutic interventions. Despite numerous new targeted immunomodulatory therapies, comprehensive approaches to apply and evaluate the effects of these treatments longitudinally are lacking. Here, we leveraged advances in programmable-phage immunoprecipitation methodology to explore the modulation, or lack thereof, of autoantibody profiles, proteome-wide, in both health and disease. Using a custom set of over 730,000 human-derived peptides, we demonstrated that each individual, regardless of disease state, possesses a distinct and complex constellation of autoreactive antibodies. For each individual, the set of resulting autoreactivites constituted a unique immunological fingerprint, or "autoreactome," that was remarkably stable over years. Using the autoreactome as a primary output, we evaluated the relative effectiveness of various immunomodulatory therapies in altering autoantibody repertoires. We found that therapies targeting B cell maturation antigen (BCMA) profoundly altered an individual's autoreactome, while anti-CD19 and anti-CD20 therapies had minimal effects. These data both confirm that the autoreactome comprises autoantibodies secreted by plasma cells and strongly suggest that BCMA or other plasma cell-targeting therapies may be highly effective in treating currently refractory autoantibody-mediated diseases.
Keywords: Adaptive immunity; Autoimmune diseases; Autoimmunity; Immunotherapy; Therapeutics.
Figures
References
MeSH terms
Substances
Grants and funding
- U2C TR002818/TR/NCATS NIH HHS/United States
- R21 AI164590/AI/NIAID NIH HHS/United States
- R01 AR073938/AR/NIAMS NIH HHS/United States
- RF1 AG032289/AG/NIA NIH HHS/United States
- P30 AG062422/AG/NIA NIH HHS/United States
- R01 AG072475/AG/NIA NIH HHS/United States
- R01 AI114780/AI/NIAID NIH HHS/United States
- R01 AG032289/AG/NIA NIH HHS/United States
- U01 CA247548/CA/NCI NIH HHS/United States
- R21 AI142198/AI/NIAID NIH HHS/United States
- U54 NS115054/NS/NINDS NIH HHS/United States
- UL1 TR001863/TR/NCATS NIH HHS/United States
- T32 GM141323/GM/NIGMS NIH HHS/United States
- R01 AR075813/AR/NIAMS NIH HHS/United States
- K12 HD000850/HD/NICHD NIH HHS/United States
LinkOut - more resources
Full Text Sources
Research Materials
