

Preclinical Study of Pulsed Field Ablation of Difficult Ventricular Targets: Intracavitary Mobile Structures, Interventricular Septum, and Left Ventricular Free Wall
- PMID: 38753535
- PMCID: PMC11186713
- DOI: 10.1161/CIRCEP.124.012734
Preclinical Study of Pulsed Field Ablation of Difficult Ventricular Targets: Intracavitary Mobile Structures, Interventricular Septum, and Left Ventricular Free Wall
Abstract
Background: Endocardial catheter-based pulsed field ablation (PFA) of the ventricular myocardium is promising. However, little is known about PFA's ability to target intracavitary structures, epicardium, and ways to achieve transmural lesions across thick ventricular tissue.
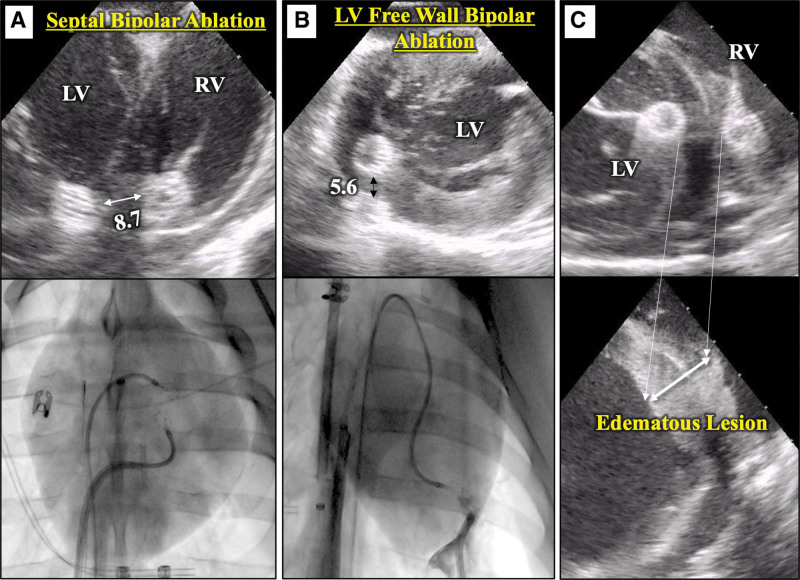
Methods: A lattice-tip catheter was used to deliver biphasic monopolar PFA to swine ventricles under general anesthesia, with electroanatomical mapping, fluoroscopy and intracardiac echocardiography guidance. We conducted experiments to assess the feasibility and safety of repetitive monopolar PFA applications to ablate (1) intracavitary papillary muscles and moderator bands, (2) epicardial targets, and (3) bipolar PFA for midmyocardial targets in the interventricular septum and left ventricular free wall.
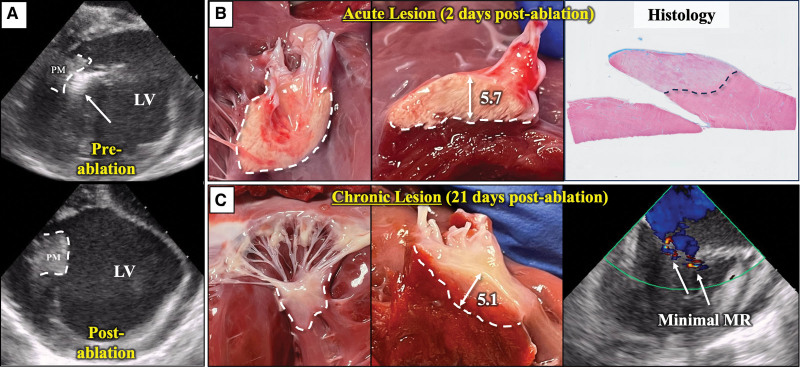
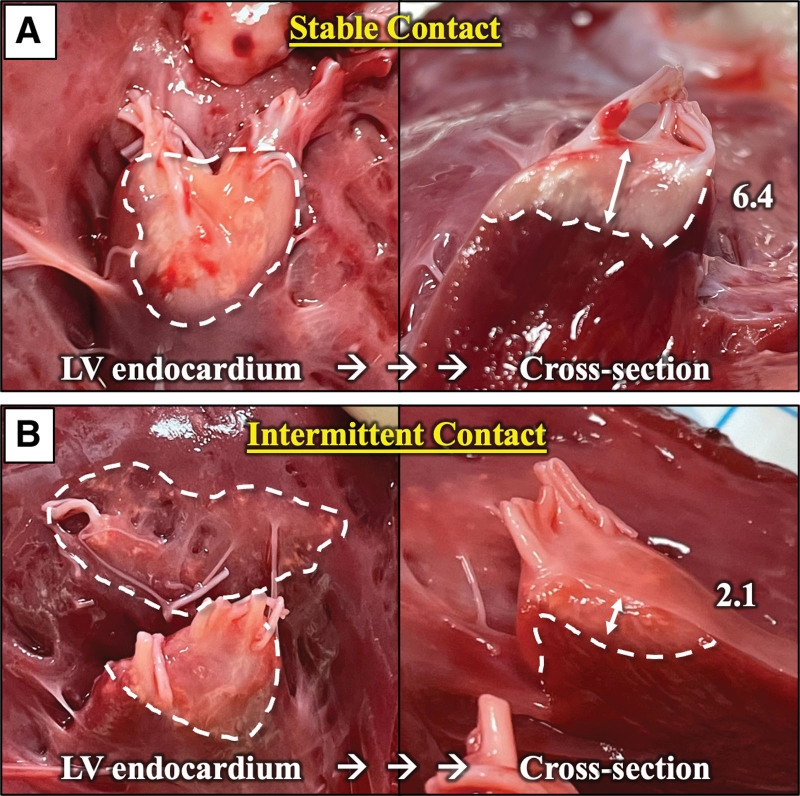
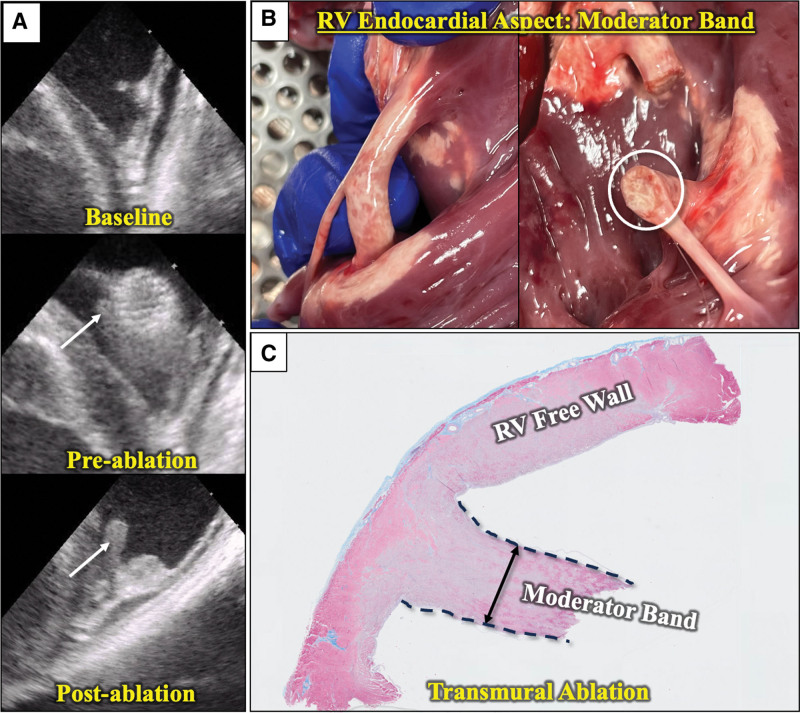
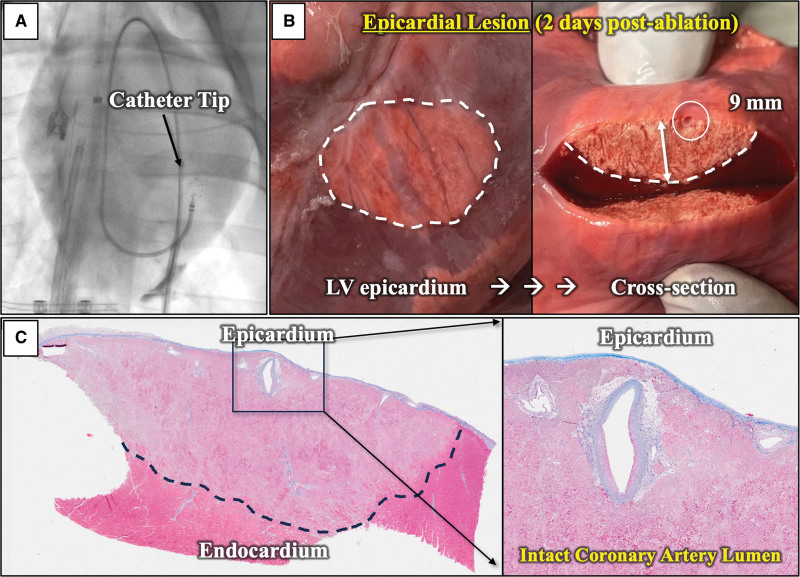
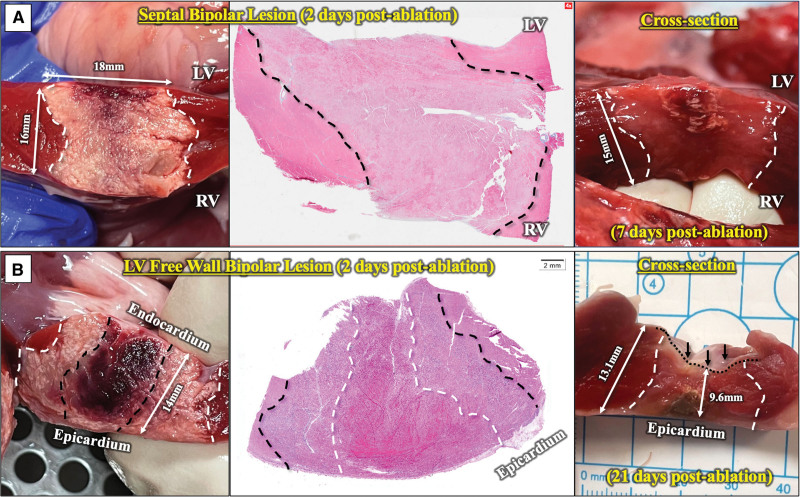
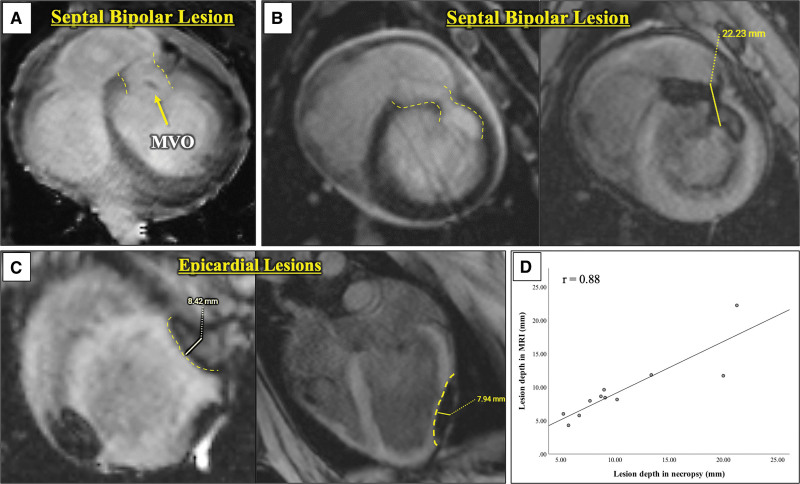
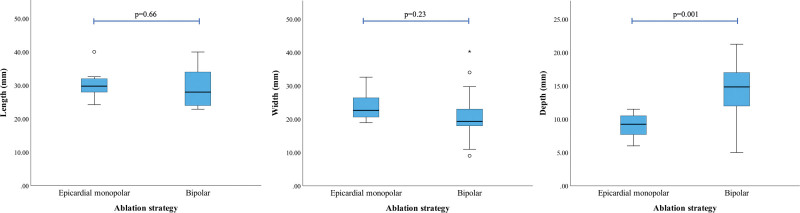
Results: (1) Papillary muscles (n=13) were successfully ablated and then evaluated at 2, 7, and 21 days. Nine lesions with stable contact measured 18.3±2.4 mm long, 15.3±1.5 mm wide, and 5.8±1.0 mm deep at 2 days. Chronic lesions demonstrated preserved chordae without mitral regurgitation. Two targeted moderator bands were transmurally ablated without structural disruption. (2) Transatrial saline/carbon dioxide assisted epicardial access was obtained successfully and epicardial monopolar lesions had a mean length, width, and depth of 30.4±4.2, 23.5±4.1, and 9.1±1.9 mm, respectively. (3) Bipolar PFA lesions were delivered across the septum (n=11) and the left ventricular free wall (n=7). Twelve completed bipolar lesions had a mean length, width, and depth of 29.6±5.5, 21.0±7.3, and 14.3±4.7 mm, respectively. Chronically, these lesions demonstrated uniform fibrotic changes without tissue disruption. Bipolar lesions were significantly deeper than the monopolar epicardial lesions.
Conclusions: This in vivo evaluation demonstrates that PFA can successfully ablate intracavitary structures and create deep epicardial lesions and transmural left ventricular lesions.
Keywords: catheter ablation; electroporation; heart ventricles; papillary muscles; swine; tachycardia, ventricular.
Conflict of interest statement
Figures
References
-
- Della Bella P, Baratto F, Tsiachris D, Trevisi N, Vergara P, Bisceglia C, Petracca F, Carbucicchio C, Benussi S, Maisano F, et al. Management of ventricular tachycardia in the setting of a dedicated unit for the treatment of complex ventricular arrhythmias: long-term outcome after ablation. Circulation. 2013;127:1359–1368. doi: 10.1161/CIRCULATIONAHA.112.000872 - PubMed
-
- Wasmer K, Reinecke H, Heitmann M, Dechering DG, Reinke F, Lange PS, Frommeyer G, Kochhauser S, Leitz P, Eckardt L, et al. Clinical, procedural and long-term outcome of ischemic VT ablation in patients with previous anterior versus inferior myocardial infarction. Clin Res Cardiol. 2020;109:1282–1291. doi: 10.1007/s00392-020-01622-z - PMC - PubMed
-
- Yamashita S, Cochet H, Sacher F, Mahida S, Berte B, Hooks D, Sellal JM, Al Jefairi N, Frontera A, Komatsu Y, et al. Impact of new technologies and approaches for post-myocardial infarction ventricular tachycardia ablation during long-term follow-up. Circ Arrhythm Electrophysiol. 2016;9:e003901. doi: 10.1161/CIRCEP.116.003901 - PubMed
-
- Barkagan M, Leshem E, Shapira-Daniels A, Sroubek J, Buxton AE, Saffitz JE, Anter E. Histopathological characterization of radiofrequency ablation in ventricular scar Tissue. JACC Clin Electrophysiol. 2019;5:920–931. doi: 10.1016/j.jacep.2019.05.011 - PubMed
-
- Schwartzman D, Chang I, Michele JJ, Mirotznik MS, Foster KR. Electrical impedance properties of normal and chronically infarcted left ventricular myocardium. J Interv Card Electrophysiol. 1999;3:213–224. doi: 10.1023/a:1009887306055 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
