

Low-Dose Aspirin Is the Safest Prophylaxis for Prevention of Venous Thromboembolism After Total Knee Arthroplasty Across All Patient Risk Profiles
- PMID: 38753809
- PMCID: PMC11254562
- DOI: 10.2106/JBJS.23.01158
Low-Dose Aspirin Is the Safest Prophylaxis for Prevention of Venous Thromboembolism After Total Knee Arthroplasty Across All Patient Risk Profiles
Abstract
Background: The International Consensus Meeting on Venous Thromboembolism (ICM-VTE) in 2022 proclaimed low-dose aspirin as the most effective agent in patients across all risk profiles undergoing joint arthroplasty. However, data on large patient populations assessing trends in chemoprophylactic choices and related outcomes following total knee arthroplasty (TKA) remain scant. The present study was designed to characterize the clinical use of various chemoprophylactic agents in patients undergoing TKA and to determine the efficacy of aspirin compared with other agents in patient groups stratified by VTE risk profiles.
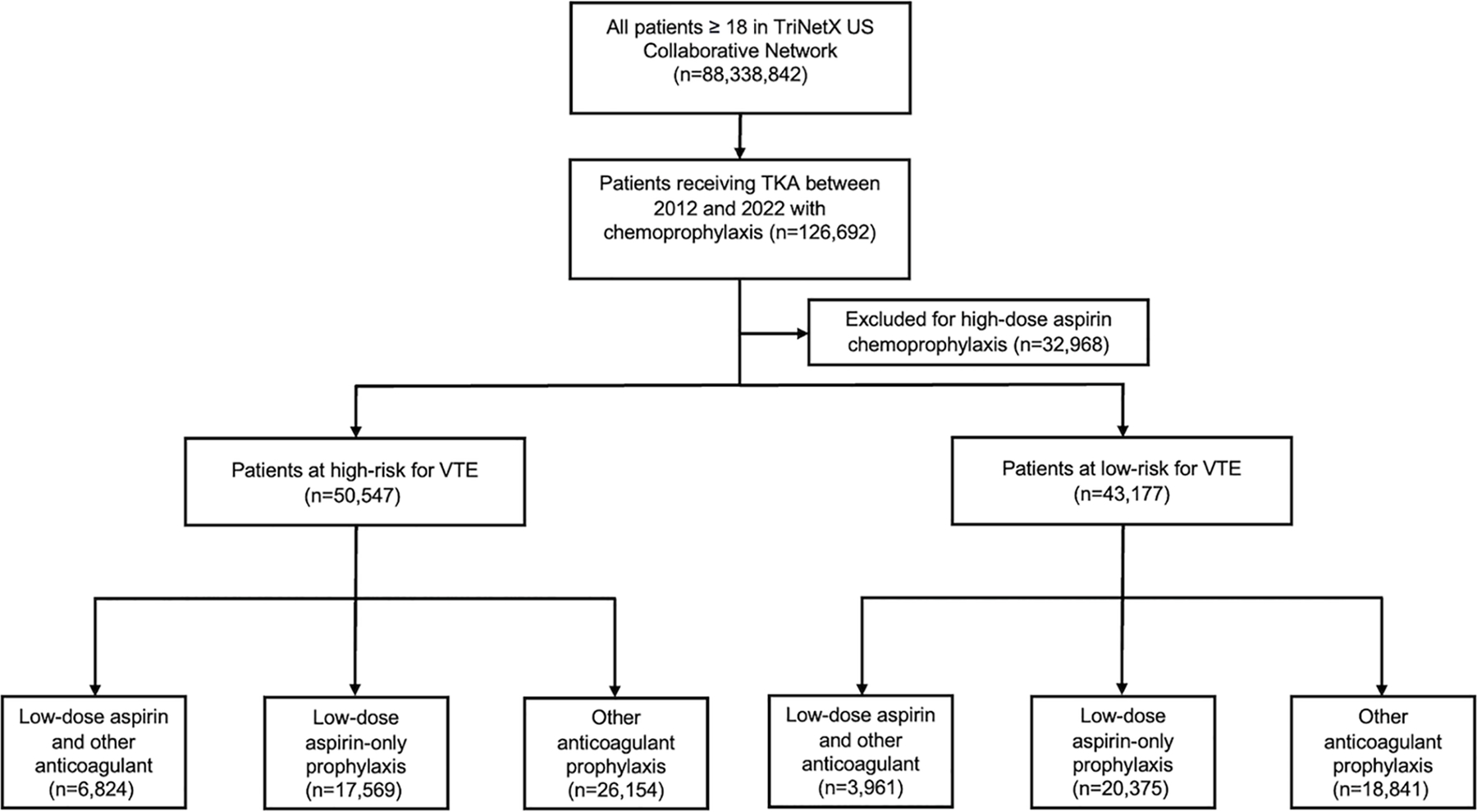
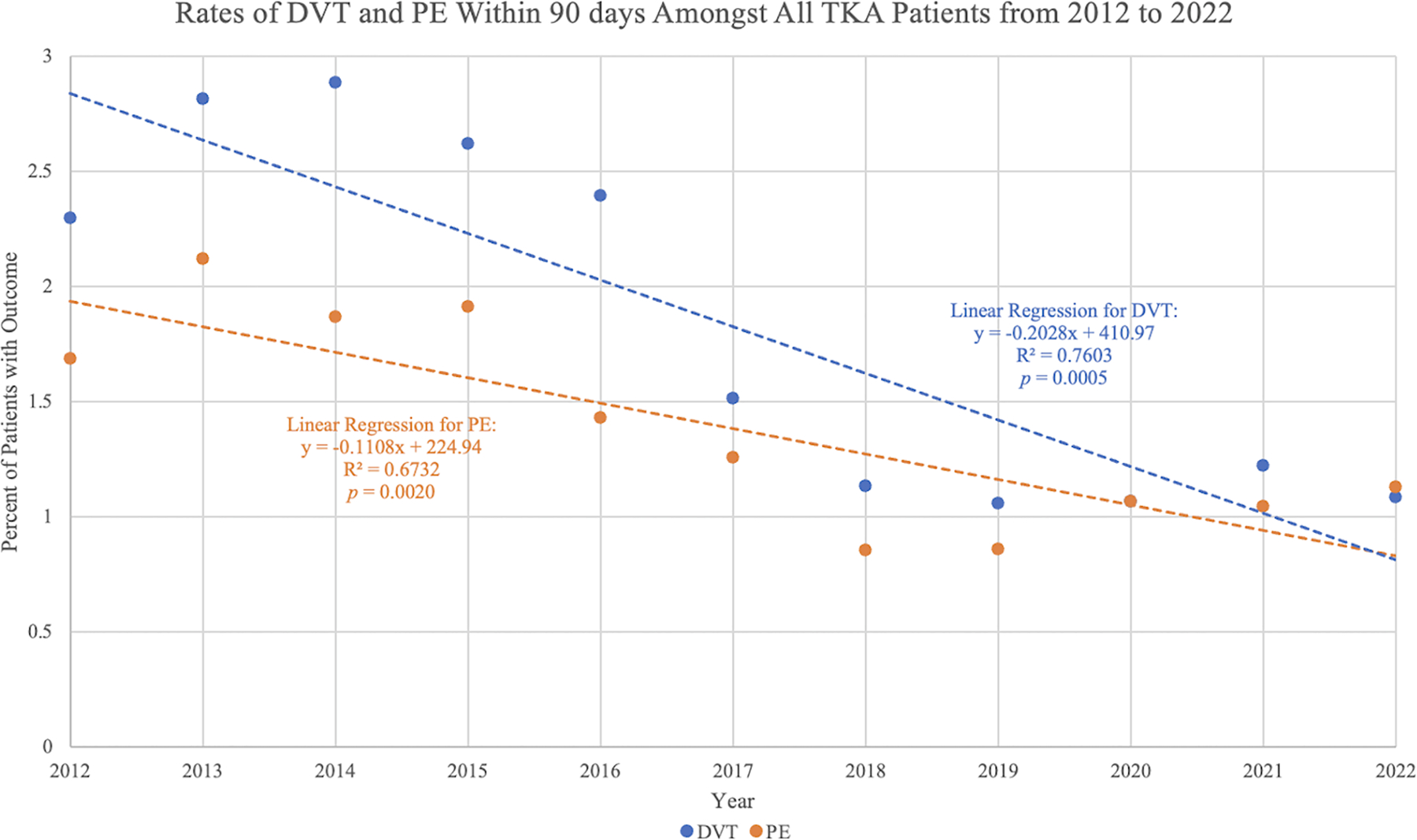
Methods: This study utilized a national database to determine the proportion of patients undergoing TKA who received low-dose aspirin versus other chemoprophylaxis between 2012 and 2022. VTE risk profiles were determined on the basis of comorbidities established in the ICM-VTE. The odds ratios (ORs) and 95% confidence intervals (CIs) between various classes of thromboprophylaxis in patients with high and low risk of VTE were calculated. The odds of deep-vein thrombosis (DVT), pulmonary embolus (PE), bleeding events, infections, mortality, and hospitalizations were also assessed in the 90-day postoperative period for propensity-matched cohorts receiving low-dose (81 mg) aspirin only versus other prophylaxis, segregating patients by VTE risk profile.
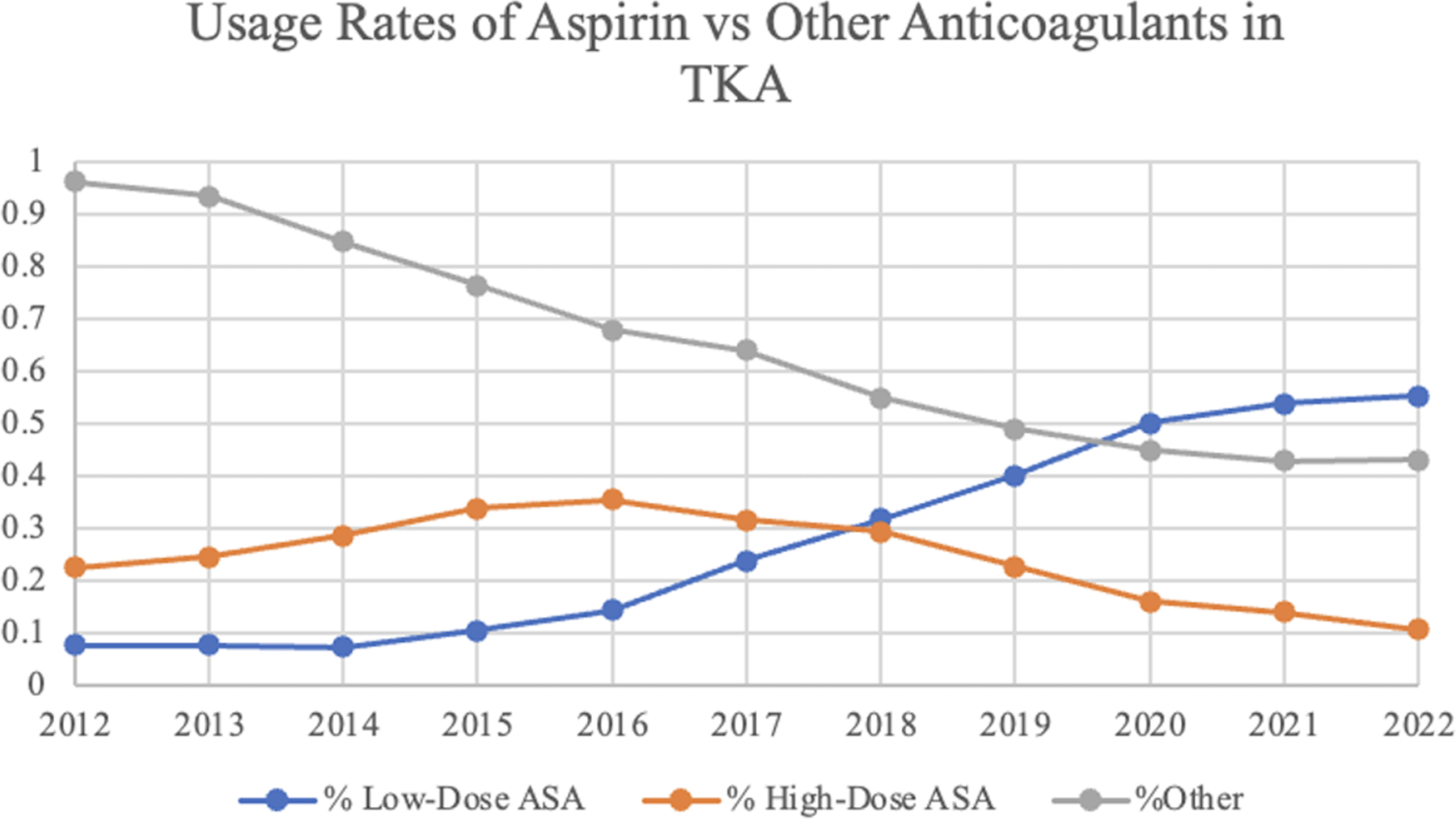
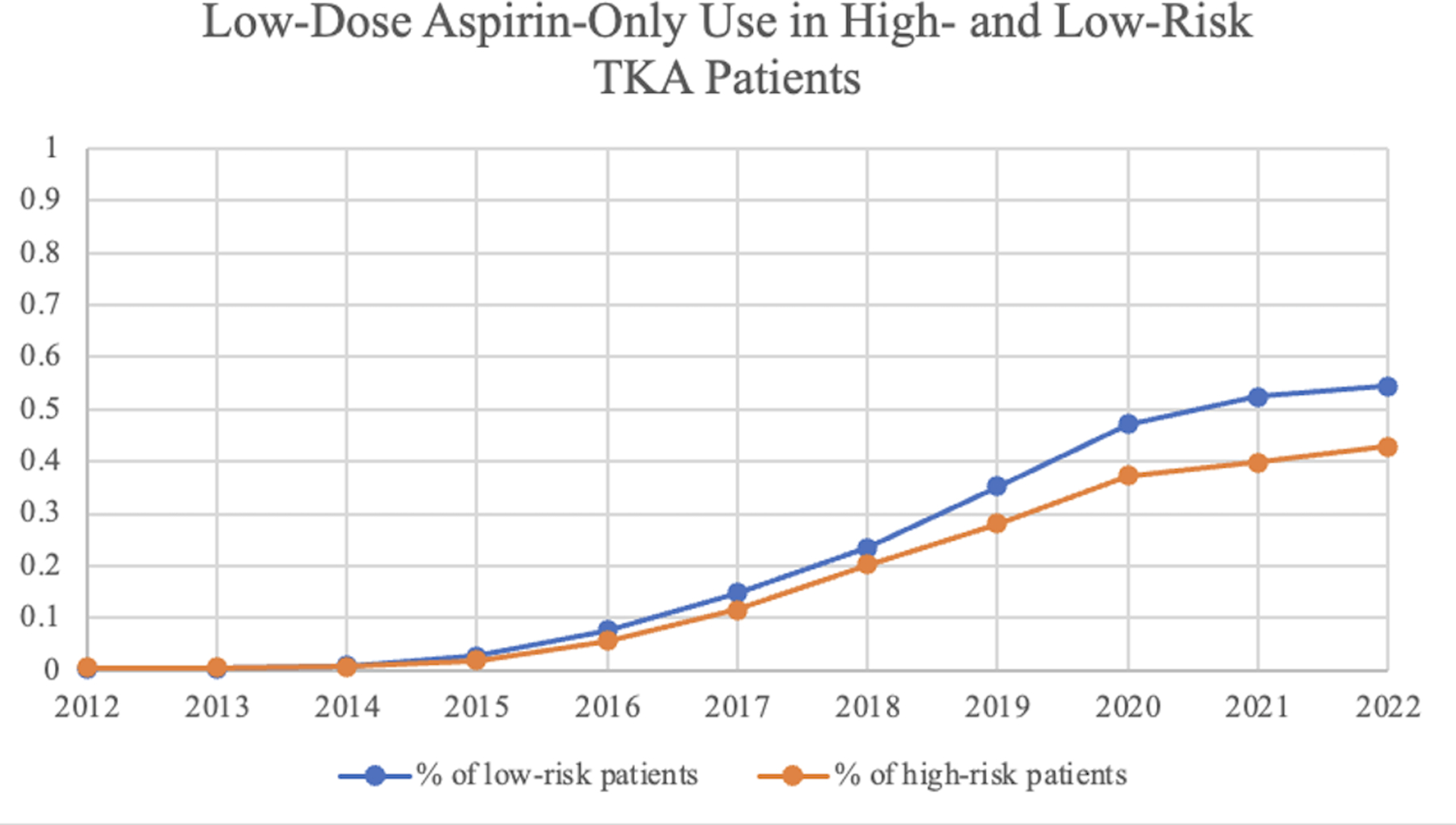
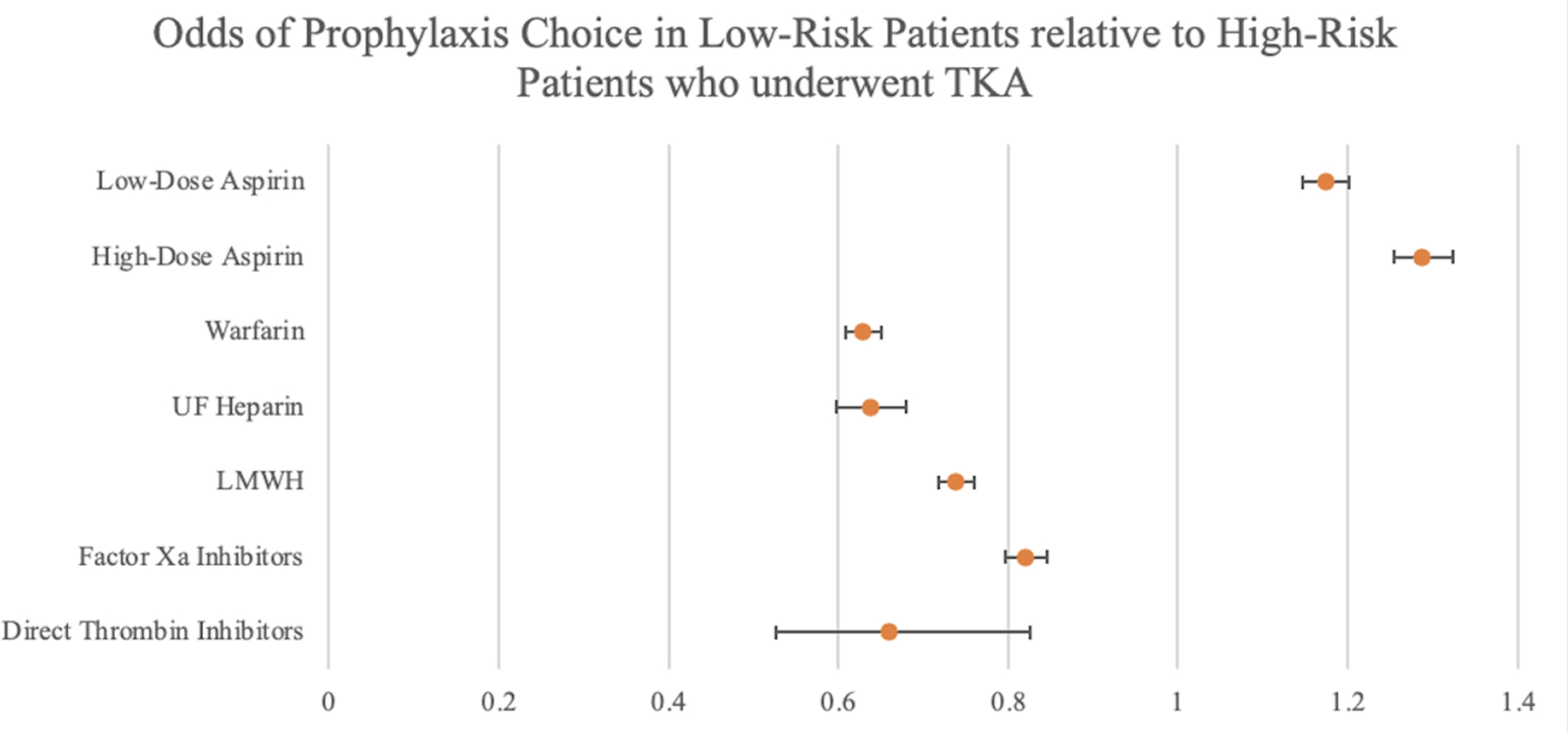
Results: A total of 126,692 patients undergoing TKA across 60 health-care organizations were included. The proportion of patients receiving low-dose aspirin increased from 7.65% to 55.29% between 2012 and 2022, whereas the proportion of patients receiving other chemoprophylaxis decreased from 96.25% to 42.98%. Low-dose-aspirin-only use increased to approximately 50% in both high-risk and low-risk populations but was more likely in low-risk populations (OR, 1.17; 95% CI, 1.15 to 1.20) relative to high-risk populations. Both low-risk and high-risk patients in the low-dose-aspirin-only cohorts had decreased odds of DVT, PE, bleeding, infections, and hospitalizations compared with other prophylaxis regimens.
Conclusions: The findings of the present study on a very large population of patients undergoing TKA support the recent ICM-VTE statement by showing that low-dose aspirin is a safe and effective method of prophylaxis in patients across various risk profiles.
Level of evidence: Therapeutic Level III . See Instructions for Authors for a complete description of levels of evidence.
Copyright © 2024 by The Journal of Bone and Joint Surgery, Incorporated.
Conflict of interest statement
Disclosure: This project was supported by the Clinical and Translational Science Collaborative (CTSC) of Cleveland, which is funded by the National Institutes of Health (NIH), National Center for Advancing Translational Science (NCATS), Clinical and Translational Science Award (CTSA) grant UL1TR002548. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH. The Disclosure of Potential Conflicts of Interest forms are provided with the online version of the article ( http://links.lww.com/JBJS/I16 ).
Figures
Similar articles
-
Aspirin Is as Effective and Safe as Oral Anticoagulants for Venous Thromboembolism Prophylaxis After Joint Arthroplasty: A Systematic Review and Meta-Analysis of Randomized Clinical Trials.J Bone Joint Surg Am. 2025 Apr 2;107(7):760-770. doi: 10.2106/JBJS.24.00946. Epub 2025 Jan 21. J Bone Joint Surg Am. 2025. PMID: 39836735 Free PMC article.
-
Anticoagulants (extended duration) for prevention of venous thromboembolism following total hip or knee replacement or hip fracture repair.Cochrane Database Syst Rev. 2016 Mar 30;3(3):CD004179. doi: 10.1002/14651858.CD004179.pub2. Cochrane Database Syst Rev. 2016. PMID: 27027384 Free PMC article.
-
Pentasaccharides for the prevention of venous thromboembolism.Cochrane Database Syst Rev. 2016 Oct 31;10(10):CD005134. doi: 10.1002/14651858.CD005134.pub3. Cochrane Database Syst Rev. 2016. PMID: 27797404 Free PMC article.
-
Screening for thrombophilia in high-risk situations: systematic review and cost-effectiveness analysis. The Thrombosis: Risk and Economic Assessment of Thrombophilia Screening (TREATS) study.Health Technol Assess. 2006 Apr;10(11):1-110. doi: 10.3310/hta10110. Health Technol Assess. 2006. PMID: 16595080
-
Low-versus high-dose aspirin for venous thromboembolic prophylaxis after total joint arthroplasty: a systematic review and meta-analysis.J Orthop Surg Res. 2024 Dec 19;19(1):848. doi: 10.1186/s13018-024-05356-w. J Orthop Surg Res. 2024. PMID: 39702480 Free PMC article.
Cited by
-
Chronic Anticoagulation is Associated With Significantly Increased Rates of Medical Complications, Periprosthetic Joint Infection, and Revision After Primary Total Knee Arthroplasty.Arthroplast Today. 2025 Jun 16;34:101749. doi: 10.1016/j.artd.2025.101749. eCollection 2025 Aug. Arthroplast Today. 2025. PMID: 40599325 Free PMC article.
-
Risk-Stratified Venous Thromboembolism Chemoprophylaxis After Total Joint Arthroplasty: Evaluation of an Institutional Approach.J Clin Med. 2025 Jan 9;14(2):366. doi: 10.3390/jcm14020366. J Clin Med. 2025. PMID: 39860378 Free PMC article.
-
The Fragility of Statistical Significance in the Use of Aspirin in Prevention of Venous Thromboembolism Events Following Total Joint Arthroplasty: Systematic Review and Meta-Analysis of Randomized Controlled Trials.J Clin Med. 2024 Oct 24;13(21):6369. doi: 10.3390/jcm13216369. J Clin Med. 2024. PMID: 39518508 Free PMC article. Review.
-
The Impact of Contemporary Glucagon-like Peptide-1 Receptor Agonists on the Onset, Severity, and Conversion to Arthroplasty in Hip and Knee Osteoarthritis.Orthop J Sports Med. 2025 Jan 13;13(1):23259671241297157. doi: 10.1177/23259671241297157. eCollection 2025 Jan. Orthop J Sports Med. 2025. PMID: 39811151 Free PMC article.
-
The Effect of Chronic Anticoagulation on Early Postoperative Outcomes Following Total Knee Arthroplasty: A TriNetX Database Study.Arthroplast Today. 2025 Apr 26;33:101690. doi: 10.1016/j.artd.2025.101690. eCollection 2025 Jun. Arthroplast Today. 2025. PMID: 40342539 Free PMC article.
References
-
- The ICM-VTE Hip & Knee Delegates. Recommendations from the ICM-VTE: Hip & Knee. J Bone Joint Surg Am. 2022. Mar 16;104(Suppl 1):180–231. - PubMed
-
- Streiff MB, Haut ER. The CMS ruling on venous thromboembolism after total knee or hip arthroplasty: weighing risks and benefits. JAMA. 2009. Mar 11;301(10):1063–5. - PubMed
-
- Ansari S, Warwick D, Ackroyd CE, Newman JH. Incidence of fatal pulmonary embolism after 1,390 knee arthroplasties without routine prophylactic anticoagulation, except in high-risk cases. J Arthroplasty. 1997. Sep;12(6):599–602. - PubMed
-
- Gill SK, Pearce AR, Everington T, Rossiter ND. Mechanical prophylaxis, early mobilisation and risk stratification: as effective as drugs for low risk patients undergoing primary joint replacement. Results in 13,384 patients. Surgeon. 2020. Aug;18(4):219–25. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
