

Optimizing patient outcomes: the impact of multimodal preemptive analgesia in video-assisted thoracoscopic lobectomy
- PMID: 38754100
- PMCID: PMC11132815
- DOI: 10.1093/icvts/ivae096
Optimizing patient outcomes: the impact of multimodal preemptive analgesia in video-assisted thoracoscopic lobectomy
Abstract
Objectives: The aim of this study was to evaluate the efficacy of a multimodal preemptive analgesia management approach, specifically incorporating ultrasound-guided thoracic paravertebral block (UG-TPVB) in conjunction with intravenous analgesia, after video-assisted thoracoscopic (VATS) lobectomy under the guidance of enhanced recovery after surgery.
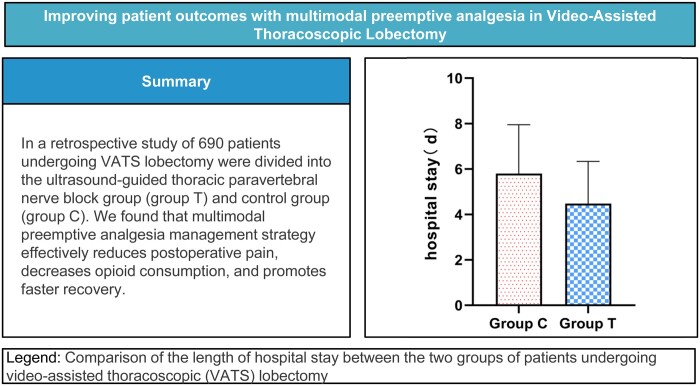
Methods: A total of 690 patients who underwent VATS lobectomy between October 2021 and March 2022 were divided into the UG-TPVB group (group T, n = 345) and the control group (group C, n = 345). Patients in group T received UG-TPVB prior to the induction of general anaesthesia, while group C did not undergo nerve block. A comparison was conducted between the 2 groups regarding various indicators, including postoperative sedation, static/dynamic numeric rating scale scores, intraoperative fentanyl consumption, duration of mechanical ventilation/anaesthesia recovery/hospitalization, postoperative complications and other relevant factors.
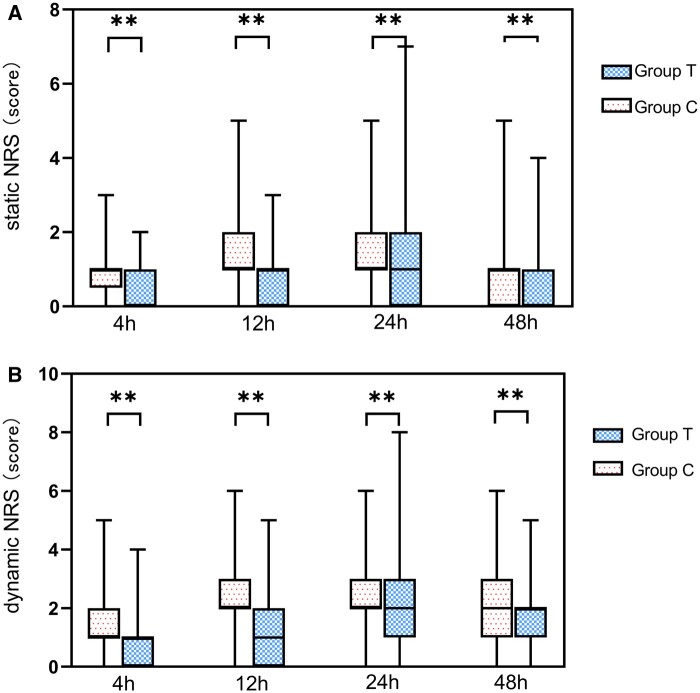
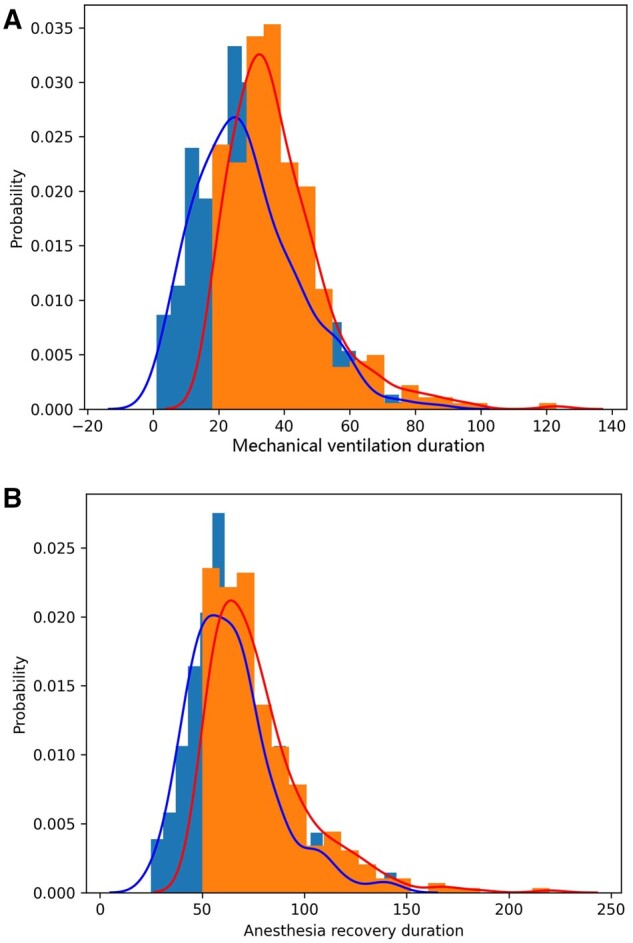
Results: The static/dynamic numeric rating scale scores of group T were lower than those of group C after surgery. Intraoperative fentanyl consumption in group T (0.384 ± 0.095 mg) was lower than that in group C (0.465 ± 0.053 mg). The duration of mechanical ventilation, anaesthesia recovery and hospitalization were significantly shorter in group T compared to group C. Patient satisfaction rate in group T (70.1%) was higher than that in group C (53.6%). All differences were statistically significant (P < 0.05).
Conclusions: The multimodal preemptive analgesia management strategy effectively reduces postoperative pain, decreases opioid consumption and promotes faster recovery in patients undergoing VATS lobectomy.
Keywords: Enhanced recovery after surgery; Intravenous analgesia; Ultrasound-guided thoracic paravertebral block; Video-assisted thoracoscopic lobectomy.
© The Author(s) 2024. Published by Oxford University Press on behalf of the European Association for Cardio-Thoracic Surgery.
Figures
Similar articles
-
Efficacy of ultrasound-guided erector spinae plane block versus paravertebral block for postoperative analgesia in single-port video-assisted thoracoscopic surgery: a retrospective study.Ann Palliat Med. 2022 Jun;11(6):1981-1989. doi: 10.21037/apm-22-75. Epub 2022 Mar 24. Ann Palliat Med. 2022. PMID: 35400156
-
Thoracic paravertebral block for perioperative lung preservation during VATS pulmonary surgery: study protocol of a randomized clinical trial.Trials. 2024 Jan 22;25(1):74. doi: 10.1186/s13063-023-07826-8. Trials. 2024. PMID: 38254233 Free PMC article.
-
Efficacy and safety of thoracoscopic-guided multiple paravertebral block for video-assisted thoracoscopic lobectomy surgery: a randomized blinded controlled study.Front Surg. 2023 Oct 24;10:1267477. doi: 10.3389/fsurg.2023.1267477. eCollection 2023. Front Surg. 2023. PMID: 37942003 Free PMC article.
-
[Multimodal Analgesia of Enhanced Recovery after Surgery Management in Lobectomy by Video-assisted Thoracoscopic Surgery].Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2021 Feb 28;43(1):136-143. doi: 10.3881/j.issn.1000-503X.12758. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2021. PMID: 33663675 Review. Chinese.
-
Enhanced recovery pathways in thoracic surgery from Italian VATS Group: perioperative analgesia protocols.J Thorac Dis. 2018 Mar;10(Suppl 4):S555-S563. doi: 10.21037/jtd.2017.12.86. J Thorac Dis. 2018. PMID: 29629202 Free PMC article. Review.
Cited by
-
Implementation of cardiac enhanced recovery after surgery at Lausanne University Hospital, our roadbook to certification.Interdiscip Cardiovasc Thorac Surg. 2024 Jul 2;39(1):ivae118. doi: 10.1093/icvts/ivae118. Interdiscip Cardiovasc Thorac Surg. 2024. PMID: 38885412 Free PMC article.
References
-
- Steinthorsdottir KJ, Wildgaard L, Hansen HJ, Petersen RH, Wildgaard K.. Regional analgesia for video-assisted thoracic surgery: a systematic review. Eur J Cardiothorac Surg 2014;45:959–66. - PubMed
-
- Xie D, Deng J, Gonzalez-Rivas D, Zhu Y, Jiang L, Jiang G. et al. Comparison of video-assisted thoracoscopic surgery with thoracotomy in bronchial sleeve lobectomy for centrally located non-small cell lung cancer. J Thorac Cardiovasc Surg 2021;161:403–13 e2. - PubMed
-
- Infante MV, Benato C, Silva R, Rocco G, Bertani A, Bertolaccini L. et al.; Italian VATS group members. What counts more: the patient, the surgical technique, or the hospital? A multivariable analysis of factors affecting perioperative complications of pulmonary lobectomy by video-assisted thoracoscopic surgery from a large nationwide registry. Eur J Cardiothorac Surg 2019;56:1209–103. - PMC - PubMed
-
- Ding W, Chen Y, Li D, Wang L, Liu H, Wang H. et al. Investigation of single-dose thoracic paravertebral analgesia for postoperative pain control after thoracoscopic lobectomy—a randomized controlled trial. Int J Surg 2018;57:8–14. - PubMed
LinkOut - more resources
Full Text Sources
