

Implementation of Inpatient Electronic Consultations During the COVID-19 Crisis and Its Sustainability Beyond the Pandemic: Quality Improvement Study
- PMID: 38754103
- PMCID: PMC11140270
- DOI: 10.2196/55623
Implementation of Inpatient Electronic Consultations During the COVID-19 Crisis and Its Sustainability Beyond the Pandemic: Quality Improvement Study
Abstract
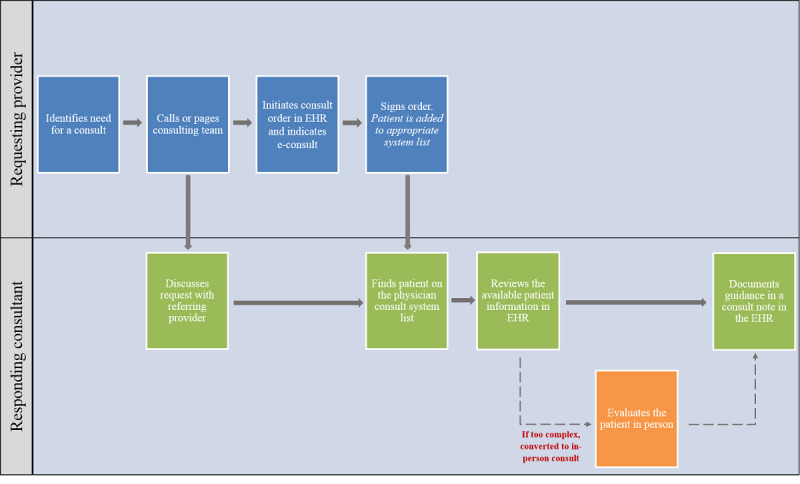
Background: Limiting in-person contact was a key strategy for controlling the spread of the highly infectious novel coronavirus (COVID-19). To protect patients and staff from the risk of infection while providing continued access to necessary health care services, we implemented a new electronic consultation (e-consult) service that allowed referring providers to receive subspecialty consultations for patients who are hospitalized and do not require in-person evaluation by the specialist.
Objective: We aimed to assess the impact of implementing e-consults in the inpatient setting to reduce avoidable face-to-face referrals during the COVID-19 pandemic.
Methods: This quality improvement study evaluated all inpatient e-consults ordered from July 2020 to December 2022 at the University of California Irvine Medical Center. The impact of e-consults was assessed by evaluating use (eg, number of e-consults ordered), e-consult response times, and outcome of the e-consult requests (eg, resolved electronically or converted to the in-person evaluation of patient).
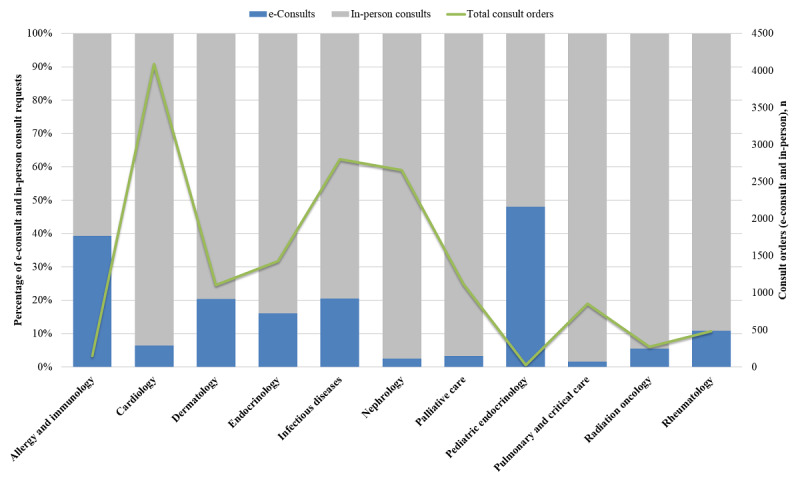
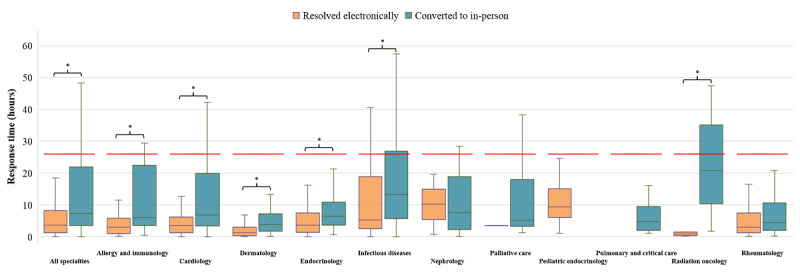
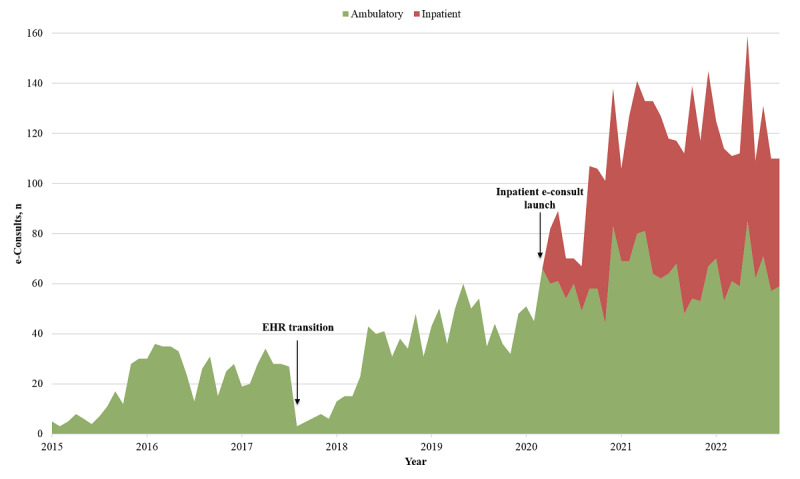
Results: There were 1543 inpatient e-consults ordered across 11 participating specialties. A total of 53.5% (n=826) of requests were addressed electronically, without the need for a formal in-person evaluation of the patient. The median time between ordering an e-consult and a specialist documenting recommendations in an e-consult note was 3.7 (IQR 1.3-8.2) hours across all specialties, contrasted with 7.3 (IQR 3.6-22.0) hours when converted to an in-person consult (P<.001). The monthly volume of e-consult requests increased, coinciding with surges of COVID-19 cases in California. After the peaks of the COVID-19 crisis subsided, the use of inpatient e-consults persisted at a rate well above the precrisis levels.
Conclusions: An inpatient e-consult service was successfully implemented, resulting in fewer unnecessary face-to-face consultations and significant reductions in the response times for consults requested on patients who are hospitalized and do not require an in-person evaluation. Thus, e-consults provided timely, efficient delivery of inpatient consultation services for appropriate problems while minimizing the risk of direct transmission of the COVID-19 virus between health care providers and patients. The service also demonstrated its value as a tool for effective inpatient care coordination beyond the peaks of the pandemic leading to the sustainability of service and value.
Keywords: COVID-19; consultations; coronavirus; e-consult; eConsult; effectiveness; electronic consultation; health care; health care providers; infectious; inpatient; novel coronavirus; pandemic; patient; patients; staff; tool; tools.
©Anna S Aledia, Amish A Dangodara, Aanya A Amin, Alpesh N Amin. Originally published in the Journal of Medical Internet Research (https://www.jmir.org), 16.05.2024.
Conflict of interest statement
Conflicts of Interest: ANA has been a principal investigator or coinvestigator of clinical trials sponsored by the National Institutes of Health/National Institute of Allergy and Infectious Diseases, NeuroRx Pharma, Pulmotect, Blade Therapeutics, Novartis, Takeda, Humanigen, Eli Lilly, PTC Therapeutics, OctaPharma, Fulcrum Therapeutics, and Alexion, as well as a speaker and consultant for BMS, Pfizer, BI, Portola, Sunovion, Mylan, Salix, Alexion, AstraZeneca, Novartis, Nabriva, Paratek, Bayer, Tetraphase, Achogen LaJolla, Ferring, Seres, Spero, Eli Lilly, Gilead, Millenium, HeartRite, Aseptiscope, and Sprightly; these relationships were unrelated to the current work. ASA, AAD, and AAA have no conflicts of interest to report.
Figures
Similar articles
-
Inpatient Electronic Consultations (E-consults) in Allergy/Immunology.J Allergy Clin Immunol Pract. 2020 Oct;8(9):2968-2973. doi: 10.1016/j.jaip.2020.06.020. Epub 2020 Jun 22. J Allergy Clin Immunol Pract. 2020. PMID: 32585408 Free PMC article.
-
Evaluation of the Effects of the COVID-19 Pandemic on Electronic Consultation Use in Primary Care.Telemed J E Health. 2022 Jan;28(1):66-72. doi: 10.1089/tmj.2020.0547. Epub 2021 Mar 31. Telemed J E Health. 2022. PMID: 33794114
-
Disruptive Innovation: Implementation of Electronic Consultations in a Veterans Affairs Health Care System.JMIR Med Inform. 2016 Feb 12;4(1):e6. doi: 10.2196/medinform.4801. JMIR Med Inform. 2016. PMID: 26872820 Free PMC article.
-
A Review of Brooke Army Medical Center Chaplaincy Service During the SARS-COV2 Pandemic: Implications for Service Structure and Patient Needs.Mil Med. 2023 Mar 20;188(3-4):e824-e828. doi: 10.1093/milmed/usab353. Mil Med. 2023. PMID: 34453171 Review.
-
Pediatric Telemedicine Consults to Improve Access to Intensive Care in Rural Environments.Pediatr Clin North Am. 2025 Feb;72(1):123-132. doi: 10.1016/j.pcl.2024.07.028. Epub 2024 Sep 26. Pediatr Clin North Am. 2025. PMID: 39603721 Review.
Cited by
-
Revolutionizing Healthcare: How Telemedicine Is Improving Patient Outcomes and Expanding Access to Care.Cureus. 2024 Jul 5;16(7):e63881. doi: 10.7759/cureus.63881. eCollection 2024 Jul. Cureus. 2024. PMID: 39099901 Free PMC article. Review.
References
-
- Keely E, Liddy C, Afkham A. Utilization, benefits, and impact of an e-consultation service across diverse specialties and primary care providers. Telemed J E Health. 2013;19(10):733–738. doi: 10.1089/tmj.2013.0007. https://europepmc.org/abstract/MED/23980939 - DOI - PMC - PubMed
-
- Malagrino GD, Chaudhry R, Gardner M, Kahn M, Speer L, Spurrier BR, LaRusso NF. A study of 6,000 electronic specialty consultations for person-centered care at The Mayo Clinic. Int J Pers Cent Med. 2012;2(3):458–466. doi: 10.5750/ijpcm.v2i3.266. - DOI
-
- Arora A, Fekieta R, Nouri Z, Carder D, Colgan MM, Fuhlbrigge A, Jackson SL, Collins S, Gleason N, Chen J. Trends in utilization of electronic consultations associated with patient payer and language among US academic medical centers during the COVID-19 pandemic. JAMA Netw Open. 2022;5(7):e2224628. doi: 10.1001/jamanetworkopen.2022.24628. https://europepmc.org/abstract/MED/35904781 2794786 - DOI - PMC - PubMed
-
- Liddy C, Moroz I, Mihan A, Nawar N, Keely E. A systematic review of asynchronous, provider-to-provider, electronic consultation services to improve access to specialty care available worldwide. Telemed J E Health. 2019;25(3):184–198. doi: 10.1089/tmj.2018.0005. https://www.liebertpub.com/doi/10.1089/tmj.2018.0005 - DOI - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
