

Modelled impact of virtual fractional flow reserve in patients undergoing coronary angiography (VIRTU-4)
- PMID: 38754969
- PMCID: PMC11287621
- DOI: 10.1136/heartjnl-2024-324039
Modelled impact of virtual fractional flow reserve in patients undergoing coronary angiography (VIRTU-4)
Abstract
Background: The practical application of 'virtual' (computed) fractional flow reserve (vFFR) based on invasive coronary angiogram (ICA) images is unknown. The objective of this cohort study was to investigate the potential of vFFR to guide the management of unselected patients undergoing ICA. The hypothesis was that it changes management in >10% of cases.
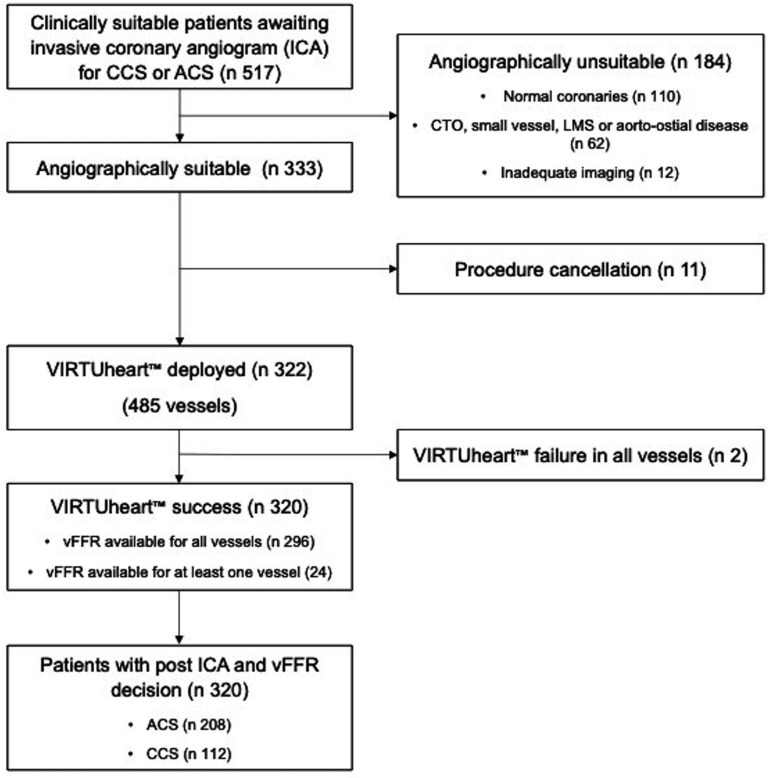
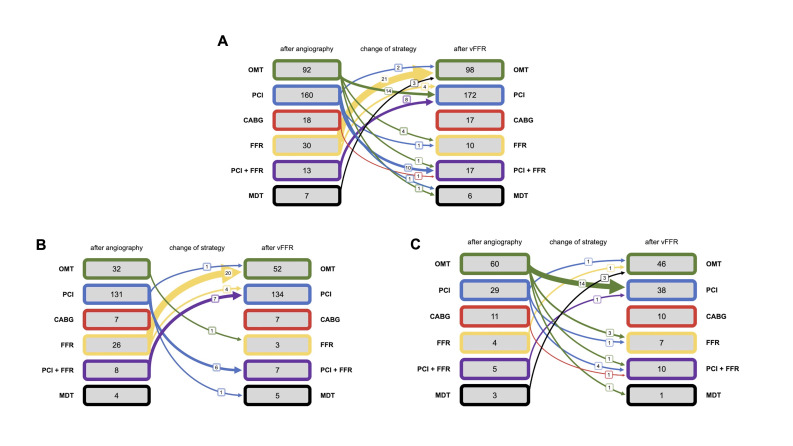
Methods: vFFR was computed using the Sheffield VIRTUheart system, at five hospitals in the North of England, on 'all-comers' undergoing ICA for non-ST-elevation myocardial infarction acute coronary syndrome (ACS) and chronic coronary syndrome (CCS). The cardiologists' management plan (optimal medical therapy, percutaneous coronary intervention (PCI), coronary artery bypass surgery or 'more information required') and confidence level were recorded after ICA, and again after vFFR disclosure.
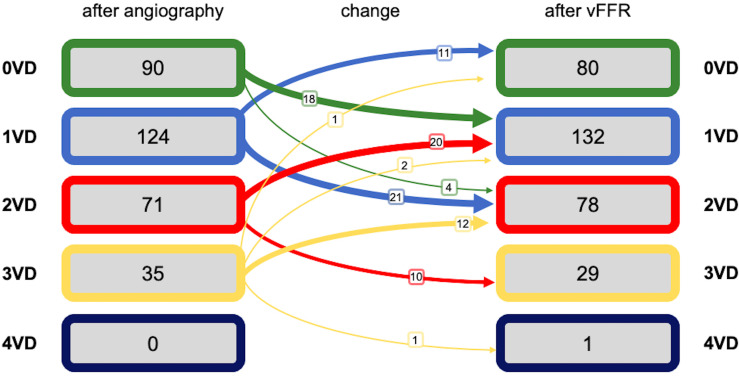
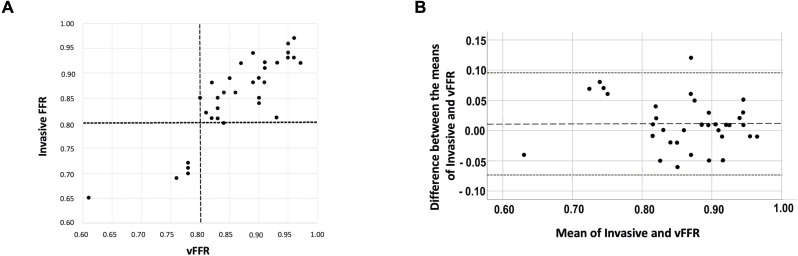
Results: 517 patients were screened; 320 were recruited: 208 with ACS and 112 with CCS. The median vFFR was 0.82 (0.70-0.91). vFFR disclosure did not change the mean number of significantly stenosed vessels per patient (1.16 (±0.96) visually and 1.18 (±0.92) with vFFR (p=0.79)). A change in intended management following vFFR disclosure occurred in 22% of all patients; in the ACS cohort, there was a 62% increase in the number planned for medical management, and in the CCS cohort, there was a 31% increase in the number planned for PCI. In all patients, vFFR disclosure increased physician confidence from 8 of 10 (7.33-9) to 9 of 10 (8-10) (p<0.001).
Conclusion: The addition of vFFR to ICA changed intended management strategy in 22% of patients, provided a detailed and specific 'all-in-one' anatomical and physiological assessment of coronary artery disease, and was accompanied by augmentation of the operator's confidence in the treatment strategy.
Keywords: Computer Simulation; Coronary Angiography; Coronary Artery Disease.
© Author(s) (or their employer(s)) 2024. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous