

Sustained IFN signaling is associated with delayed development of SARS-CoV-2-specific immunity
- PMID: 38755196
- PMCID: PMC11522391
- DOI: 10.1038/s41467-024-48556-y
Sustained IFN signaling is associated with delayed development of SARS-CoV-2-specific immunity
Abstract
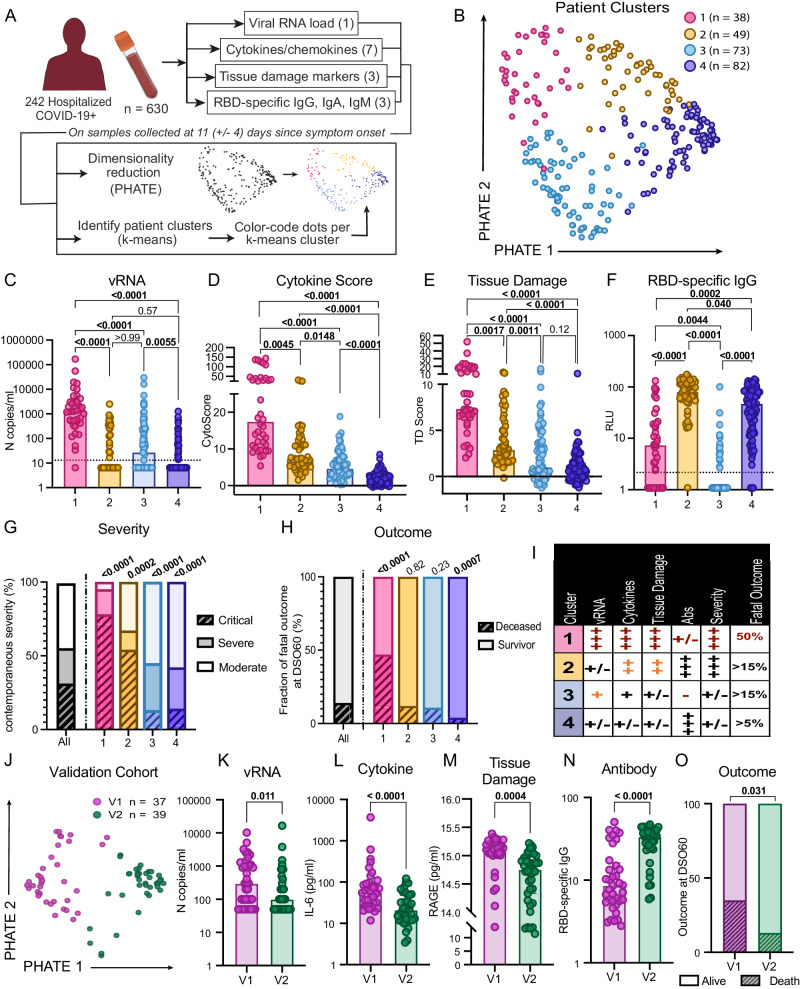
Plasma RNAemia, delayed antibody responses and inflammation predict COVID-19 outcomes, but the mechanisms underlying these immunovirological patterns are poorly understood. We profile 782 longitudinal plasma samples from 318 hospitalized patients with COVID-19. Integrated analysis using k-means reveals four patient clusters in a discovery cohort: mechanically ventilated critically-ill cases are subdivided into good prognosis and high-fatality clusters (reproduced in a validation cohort), while non-critical survivors segregate into high and low early antibody responders. Only the high-fatality cluster is enriched for transcriptomic signatures associated with COVID-19 severity, and each cluster has distinct RBD-specific antibody elicitation kinetics. Both critical and non-critical clusters with delayed antibody responses exhibit sustained IFN signatures, which negatively correlate with contemporaneous RBD-specific IgG levels and absolute SARS-CoV-2-specific B and CD4+ T cell frequencies. These data suggest that the "Interferon paradox" previously described in murine LCMV models is operative in COVID-19, with excessive IFN signaling delaying development of adaptive virus-specific immunity.
© 2024. The Author(s).
Conflict of interest statement
J.B.R. has served as an advisor to GlaxoSmithKline and Deerfield Capital. T.N. has received speaking fee from Boehringer Ingelheim for talks unrelated to this research. D.E.K. has served as an advisor to AstraZeneca. These agencies had no role in the design, implementation, or interpretation of this study. The authors declare that they have no other competing interests.
Figures




References
MeSH terms
Grants and funding
- F31 HL156419/HL/NHLBI NIH HHS/United States
- VR2-173203/Gouvernement du Canada | Instituts de Recherche en Santé du Canada | CIHR Skin Research Training Centre (Skin Research Training Centre)
- 110068-68-RGCV/amfAR, The Foundation for AIDS Research (amfAR)
- R01 GM135929/GM/NIGMS NIH HHS/United States
- 41027/Canada Foundation for Innovation (Fondation canadienne pour l'innovation)
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
