

Emergency critical care: closing the gap between onset of critical illness and intensive care unit admission
- PMID: 38755419
- PMCID: PMC11632058
- DOI: 10.1007/s00508-024-02374-w
Emergency critical care: closing the gap between onset of critical illness and intensive care unit admission
Abstract
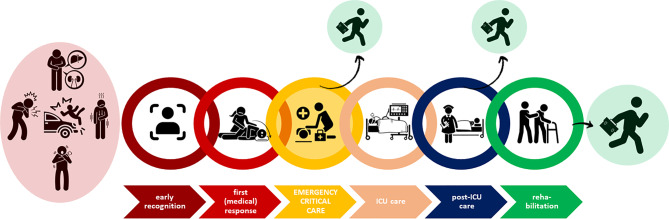
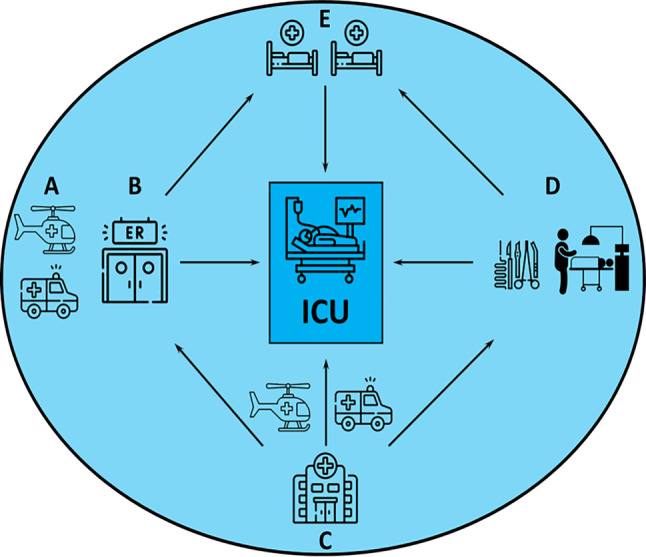
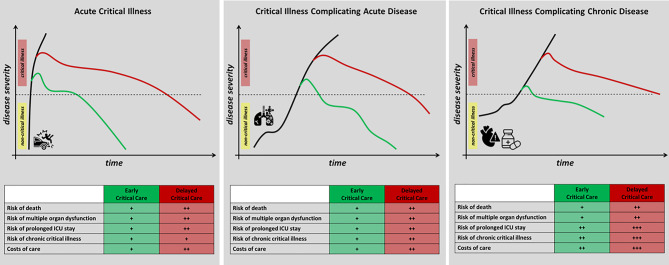
Critical illness is an exquisitely time-sensitive condition and follows a disease continuum, which always starts before admission to the intensive care unit (ICU), in the majority of cases even before hospital admission. Reflecting the common practice in many healthcare systems that critical care is mainly provided in the confined areas of an ICU, any delay in ICU admission of critically ill patients is associated with increased morbidity and mortality. However, if appropriate critical care interventions are provided before ICU admission, this association is not observed. Emergency critical care refers to critical care provided outside of the ICU. It encompasses the delivery of critical care interventions to and monitoring of patients at the place and time closest to the onset of critical illness as well as during transfer to the ICU. Thus, emergency critical care covers the most time-sensitive phase of critical illness and constitutes one missing link in the chain of survival of the critically ill patient. Emergency critical care is delivered whenever and wherever critical illness occurs such as in the pre-hospital setting, before and during inter-hospital transfers of critically ill patients, in the emergency department, in the operating theatres, and on hospital wards. By closing the management gap between onset of critical illness and ICU admission, emergency critical care improves patient safety and can avoid early deaths, reverse mild-to-moderate critical illness, avoid ICU admission, attenuate the severity of organ dysfunction, shorten ICU length of stay, and reduce short- and long-term mortality of critically ill patients. Future research is needed to identify effective models to implement emergency critical care systems in different healthcare systems.
Keywords: Critical illness; Emergency critical care; Emergency department; Medical emergency team; Prehospital.
© 2024. The Author(s).
Conflict of interest statement
Conflict of interest: M.W. Dünser, M. Noitz, T. Tschoellitsch, M. Bruckner, M. Brunner, B. Eichler, R. Erblich, S. Kalb, M. Knöll, J. Szasz, W. Behringer and J. Meier declare that they have no competing interests.
Figures

References
-
- Calvo Herranz E, Mozo MMT, Gordo VF. Introduction of a management system in intensive care medicine based on the safety of the seriously ill patient during the entire hospitalization process: extended intensive care medicine. Med Intensiva. 2011;35(6):354–60. - PubMed
-
- Bircher NG, Chan PS, Xu Y, American Heart Association. Delays in Cardiopulmonary Resuscitation, Defibrillation, and Epinephrine Administration All Decrease Survival in In-Hospital Cardiac Arrest. Anesthesiology. 2019;130(3):414–22. - PubMed
-
- Atkinson JL, Anderson RE, Murray MJ, et al. The early critical phase of severe head injury: importance of apnea and dysfunctional respiration. J Trauma. 1998;45(5:941–5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
