

Asciminib monotherapy in patients with chronic-phase chronic myeloid leukemia with the T315I mutation after ≥1 prior tyrosine kinase inhibitor: 2-year follow-up results
- PMID: 38755421
- PMCID: PMC11217003
- DOI: 10.1038/s41375-024-02278-8
Asciminib monotherapy in patients with chronic-phase chronic myeloid leukemia with the T315I mutation after ≥1 prior tyrosine kinase inhibitor: 2-year follow-up results
Abstract
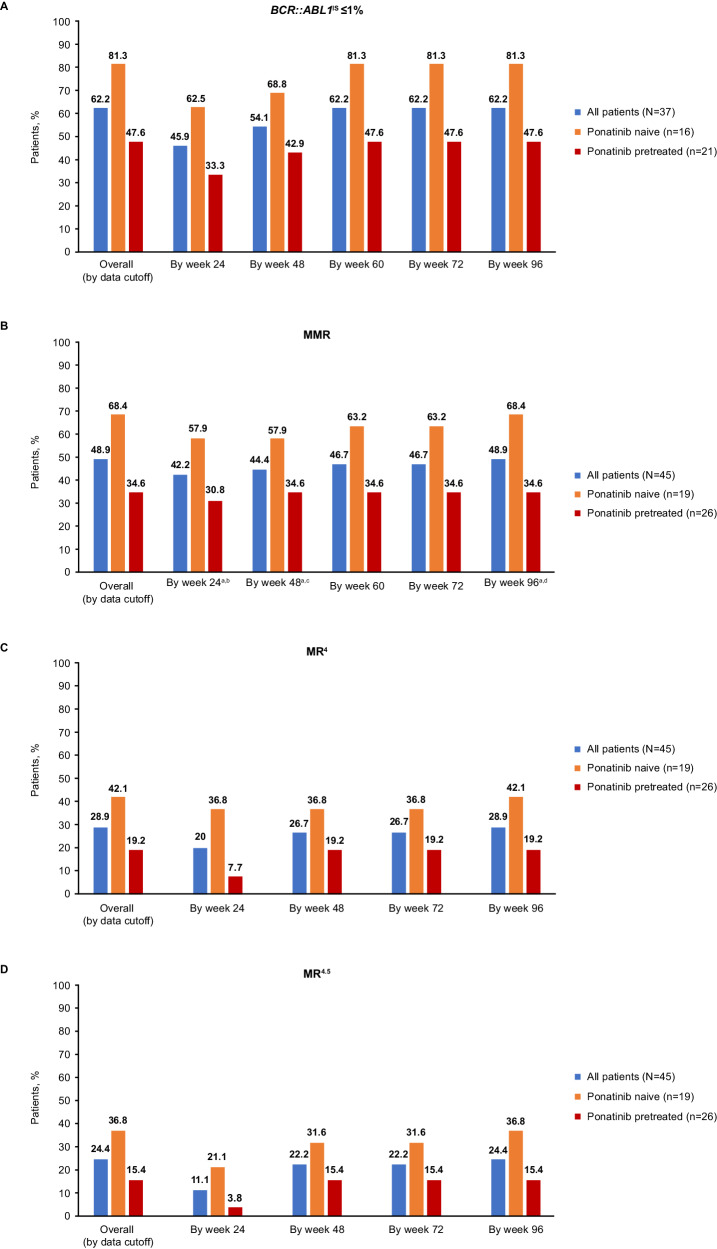
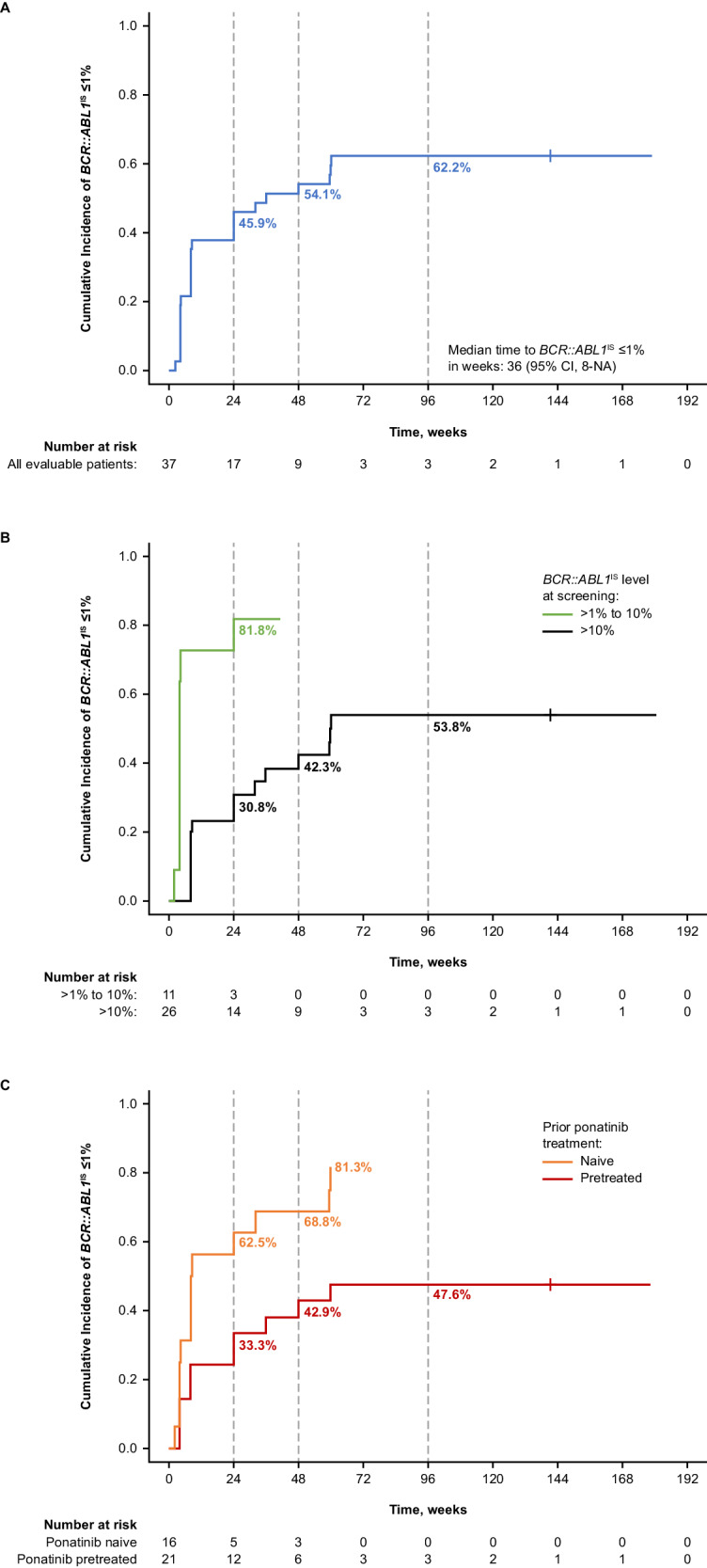
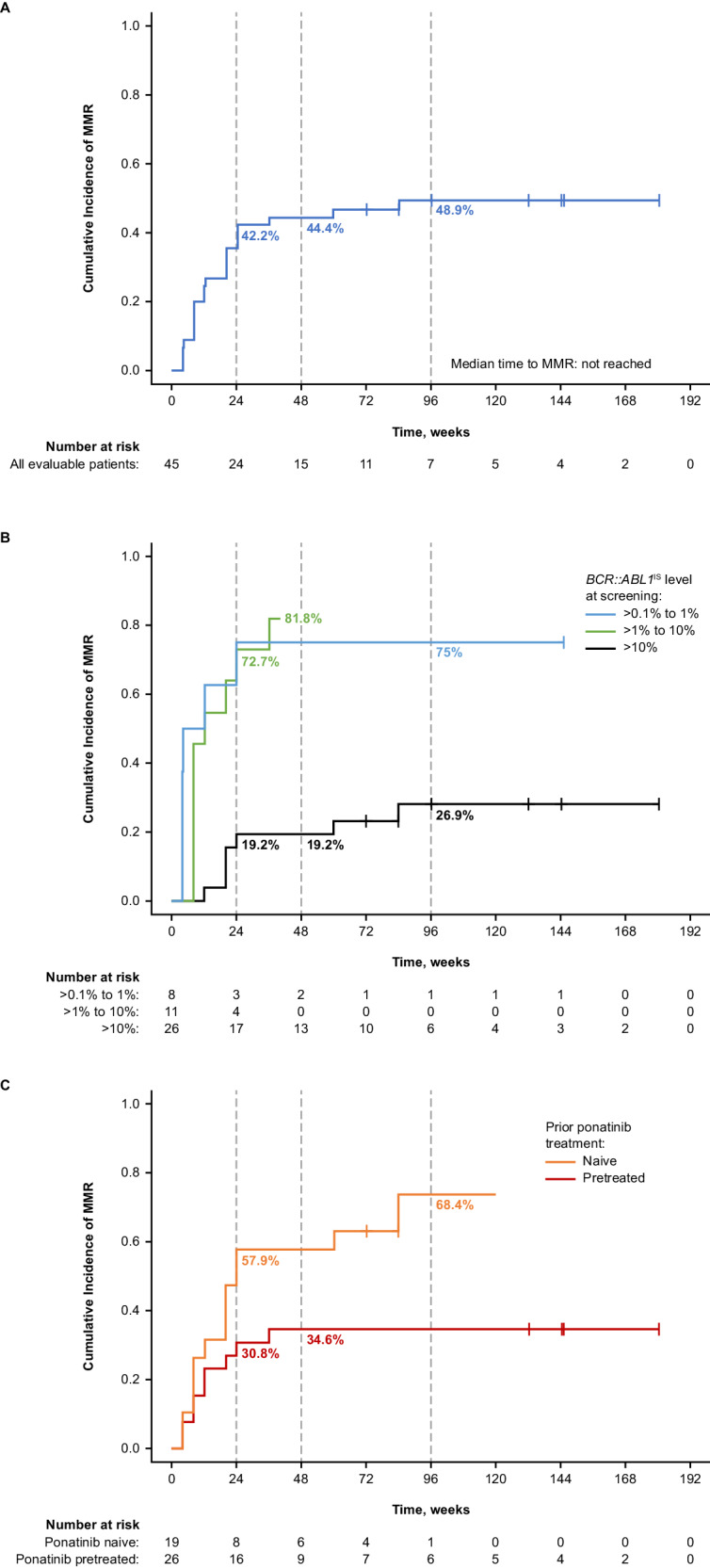
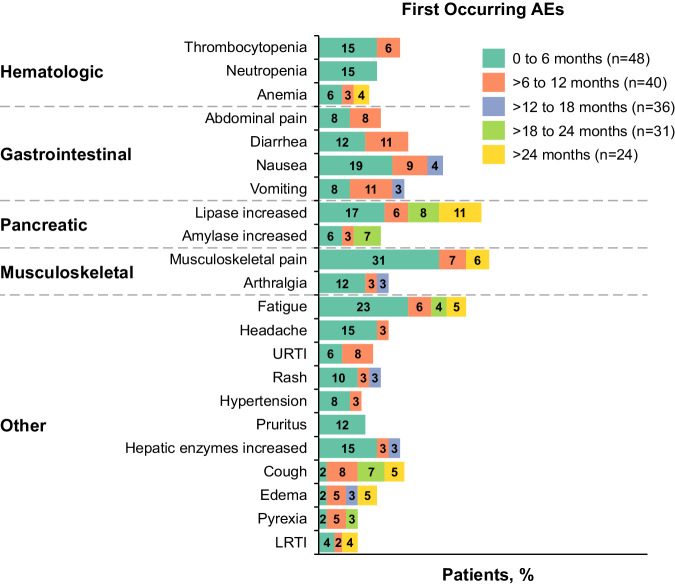
Asciminib targets the BCR::ABL1 myristoyl pocket, maintaining activity against BCR::ABL1T315I, which is resistant to most approved adenosine triphosphate-competitive tyrosine kinase inhibitors. We report updated phase I results (NCT02081378) assessing safety/tolerability and antileukemic activity of asciminib monotherapy 200 mg twice daily in 48 heavily pretreated patients with T315I-mutated chronic-phase chronic myeloid leukemia (CML-CP; data cutoff: January 6, 2021). With 2 years' median exposure, 56.3% of patients continued receiving asciminib. Overall, 62.2% of evaluable patients achieved BCR::ABL1 ≤1% on the International Scale (IS); 47.6% and 81.3% of ponatinib-pretreated and -naive patients, respectively, achieved BCR::ABL1IS ≤1%. Of 45 evaluable patients, 48.9% achieved a major molecular response (MMR, BCR::ABL1IS ≤0.1%), including 34.6% and 68.4% of ponatinib-pretreated and -naive patients, respectively. MMR was maintained until data cutoff in 19 of 22 patients who achieved it. The most common grade ≥3 adverse events (AEs) included increased lipase level (18.8%) and thrombocytopenia (14.6%). Five (10.4%) patients experienced AEs leading to discontinuation, including 2 who discontinued asciminib and died due to COVID-19; these were the only deaths reported. These results show asciminib's effectiveness, including in almost 50% of ponatinib pretreated patients, and confirm its risk-benefit profile, supporting its use as a treatment option for T315I-mutated CML-CP.
© 2024. The Author(s).
Conflict of interest statement
JEC
Figures
References
-
- Akard LP, Albitar M, Hill CE, Pinilla-Ibarz J. The “hit hard and hit early” approach to the treatment of chronic myeloid leukemia: implications of the updated National Comprehensive Cancer Network clinical practice guidelines for routine practice. Clin Adv Hematol Oncol. 2013;11:421–32.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
