

Associations of CBC-Derived inflammatory indicators with sarcopenia and mortality in adults: evidence from Nhanes 1999 ∼ 2006
- PMID: 38755603
- PMCID: PMC11100216
- DOI: 10.1186/s12877-024-05012-2
Associations of CBC-Derived inflammatory indicators with sarcopenia and mortality in adults: evidence from Nhanes 1999 ∼ 2006
Abstract
Background: It has been proposed that inflammation plays a role in the development of sarcopenia. This study aimed to investigate the links of complete blood cell count (CBC) parameters and CBC-derived inflammatory indicators with sarcopenia and mortality.
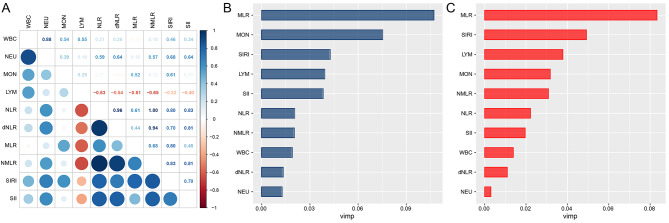
Methods: Data pertaining to sarcopenia were extracted from the 1999-2006 National Health and Nutrition Examination Survey (NHANES), and mortality events were ascertained through the National Death Index up to December 31, 2019. The CBC-derived inflammatory indicators assessed in this study included the neutrophil-to-lymphocyte ratio (NLR), derived neutrophil-to-lymphocyte ratio (dNLR), monocyte-to-lymphocyte ratio (MLR), neutrophil-monocyte to lymphocyte ratio (NMLR), systemic inflammatory response index (SIRI), and systemic immune-inflammation index (SII). The prognostic significance of these CBC-derived inflammatory indicators was evaluated using the random survival forests (RSF) analysis.
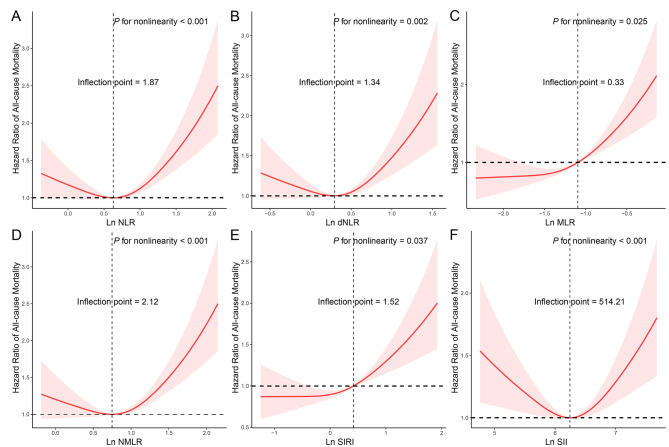
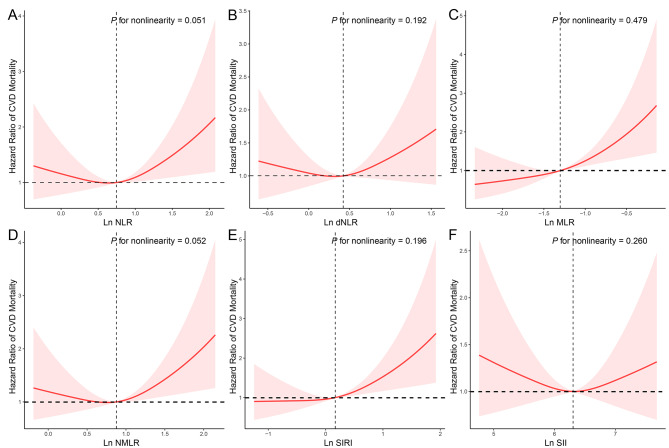
Results: The study encompassed a cohort of 12,689 individuals, among whom 1,725 were diagnosed with sarcopenia. Among individuals with sarcopenia, 782 experienced all-cause mortality, and 195 succumbed to cardiovascular causes. Following adjustment for confounding variables, it was observed that elevated levels of NLR, dNLR, NMLR, SIRI, and SII were associated with an increased prevalence of sarcopenia. Among participants with sarcopenia, those in the highest quartile of NLR (HR = 1.336 [1.095-1.631]), dNLR (HR = 1.274 [1.046-1.550]), MLR (HR = 1.619 [1.290-2.032]), NMLR (HR = 1.390 [1.132-1.707]), and SIRI (HR = 1.501 [1.210-1.862]) exhibited an elevated risk of all-cause mortality compared to those in the lowest quartile of these inflammation-derived indicators. These associations were similarly observed in cardiovascular mortality (HR = 1.874 [1.169-3.003] for MLR, HR = 1.838 [1.175-2.878] for SIRI). The RSF analysis indicated that MLR exhibited the highest predictive power for both all-cause and cardiovascular mortality among individuals with sarcopenia.
Conclusions: Our findings underscore the association between CBC-derived inflammatory indicators and mortality in adults with sarcopenia. Of note, MLR emerged as the most robust predictor of all-cause and cardiovascular mortality in this population.
Keywords: CBC-derived inflammatory indicators; Mortality; NHANES; Random survival forests; Sarcopenia.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures
Similar articles
-
The relationship between complete blood cell count-derived inflammatory biomarkers and erectile dysfunction in the United States.Sci Rep. 2024 Dec 30;14(1):32014. doi: 10.1038/s41598-024-83733-5. Sci Rep. 2024. PMID: 39738513 Free PMC article.
-
The systemic inflammation response index as risks factor for all-cause and cardiovascular mortality among individuals with respiratory sarcopenia.BMC Pulm Med. 2025 Feb 26;25(1):90. doi: 10.1186/s12890-025-03525-z. BMC Pulm Med. 2025. PMID: 40011897 Free PMC article.
-
Association between complete blood count-derived inflammatory markers and the risk of frailty and mortality in middle-aged and older adults.Front Public Health. 2024 Jul 31;12:1427546. doi: 10.3389/fpubh.2024.1427546. eCollection 2024. Front Public Health. 2024. PMID: 39145178 Free PMC article.
-
Inflammatory Hematological Indices, Cardiovascular Disease and Mortality: A Narrative Review.Arq Bras Cardiol. 2024 Aug 26;121(7):e20230752. doi: 10.36660/abc.20230752. eCollection 2024. Arq Bras Cardiol. 2024. PMID: 39193999 Free PMC article. Review. English, Portuguese.
-
Association between the systemic immune-inflammation index and sarcopenia: a systematic review and meta-analysis.J Orthop Surg Res. 2024 May 28;19(1):314. doi: 10.1186/s13018-024-04808-7. J Orthop Surg Res. 2024. PMID: 38802828 Free PMC article.
Cited by
-
The Protective Effect of Bilirubin on MAFLD May Be Mediated by Improving Insulin Re-Sistance and Alleviating Chronic Inflammation.J Inflamm Res. 2025 Apr 24;18:5555-5572. doi: 10.2147/JIR.S520257. eCollection 2025. J Inflamm Res. 2025. PMID: 40297544 Free PMC article.
-
Association of non-high-density lipoprotein cholesterol to high-density lipoprotein cholesterol (NHHR) and sarcopenia in elderly adults.Front Nutr. 2025 Jun 30;12:1614263. doi: 10.3389/fnut.2025.1614263. eCollection 2025. Front Nutr. 2025. PMID: 40661690 Free PMC article.
-
Association of cardiovascular health with MAFLD and mortality in overweight and obese adults and mediation by inflammation and insulin resistance.Sci Rep. 2025 May 29;15(1):18791. doi: 10.1038/s41598-025-03820-z. Sci Rep. 2025. PMID: 40442189 Free PMC article.
-
Relationship of monocyte to high-density lipoprotein ratio (MHR) and other inflammatory biomarkers with sarcopenia: a population-based study.Lipids Health Dis. 2025 Feb 8;24(1):42. doi: 10.1186/s12944-025-02464-2. Lipids Health Dis. 2025. PMID: 39923040 Free PMC article.
-
The association between triglyceride-glucose index, atherogenic index of plasma, systemic immune-inflammation index, and mortality in patients with acute coronary syndrome: the direct effects of glucose-lipid metabolism and U-shaped immune modulation in mortality risk.Front Cardiovasc Med. 2025 Jul 25;12:1604284. doi: 10.3389/fcvm.2025.1604284. eCollection 2025. Front Cardiovasc Med. 2025. PMID: 40787234 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
