

Construction and evaluation of short - term and long - term mortality risk prediction model for patients with sepsis based on MIMIC - IV database
- PMID: 38755721
- PMCID: PMC11103058
- DOI: 10.11817/j.issn.1672-7347.2024.230390
Construction and evaluation of short - term and long - term mortality risk prediction model for patients with sepsis based on MIMIC - IV database
Abstract
Objectives: Given the high incidence and mortality rate of sepsis, early identification of high-risk patients and timely intervention are crucial. However, existing mortality risk prediction models still have shortcomings in terms of operation, applicability, and evaluation on long-term prognosis. This study aims to investigate the risk factors for death in patients with sepsis, and to construct the prediction model of short-term and long-term mortality risk.
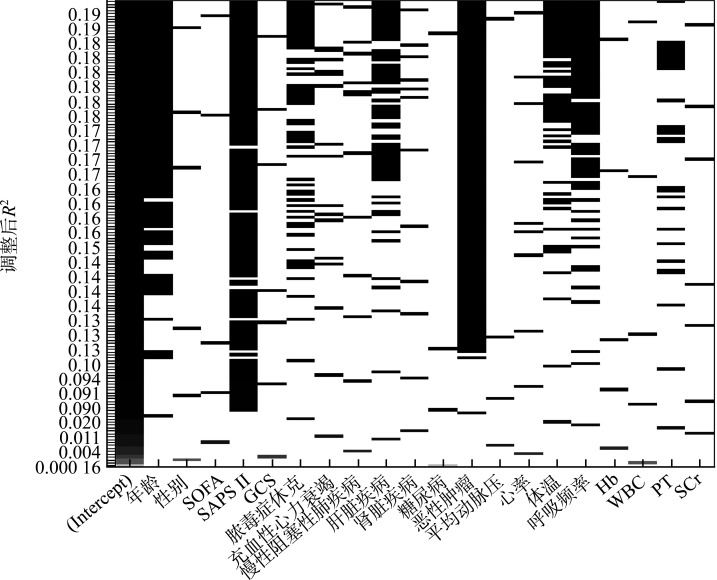
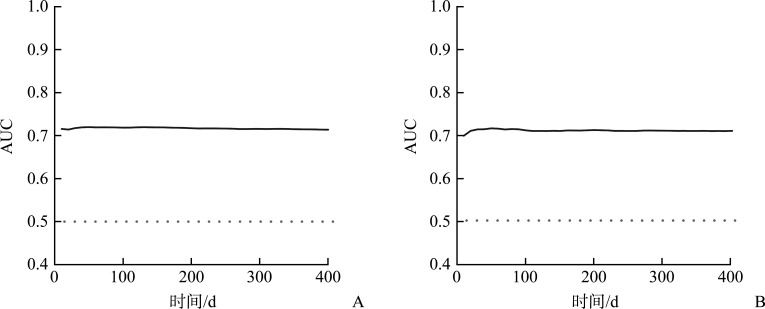
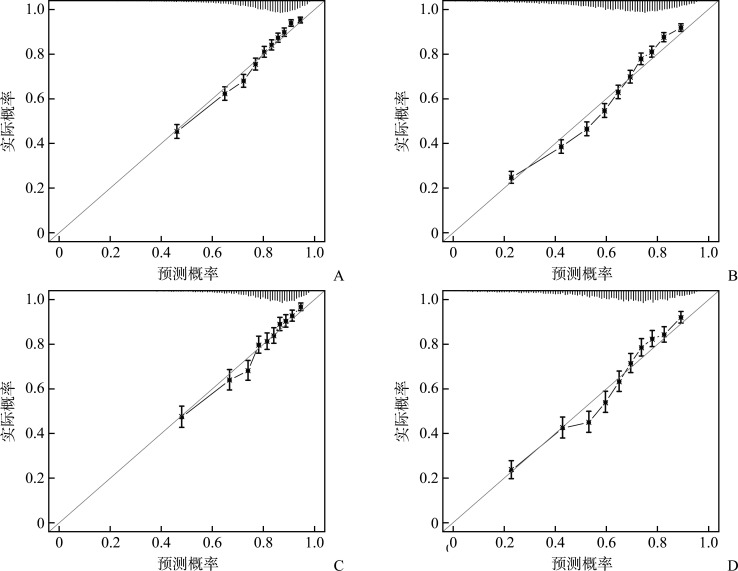
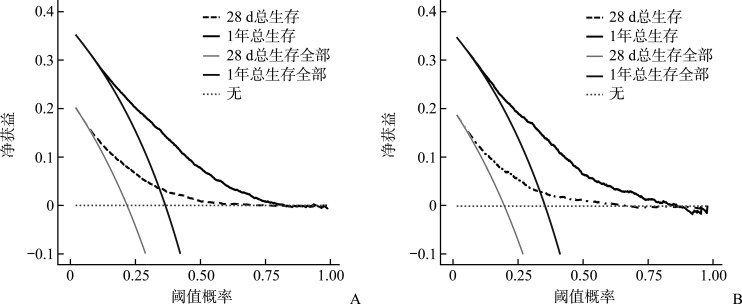
Methods: Patients meeting sepsis 3.0 diagnostic criteria were selected from the Medical Information Mart for Intensive Care-IV (MIMIC-IV) database and randomly divided into a modeling group and a validation group at a ratio of 7꞉3. Baseline data of patients were analyzed. Univariate Cox regression analysis and full subset regression were used to determine the risk factors of death in patients with sepsis and to screen out the variables to construct the prediction model. The time-dependent area under the curve (AUC), calibration curve, and decision curve were used to evaluate the differentiation, calibration, and clinical practicability of the model.
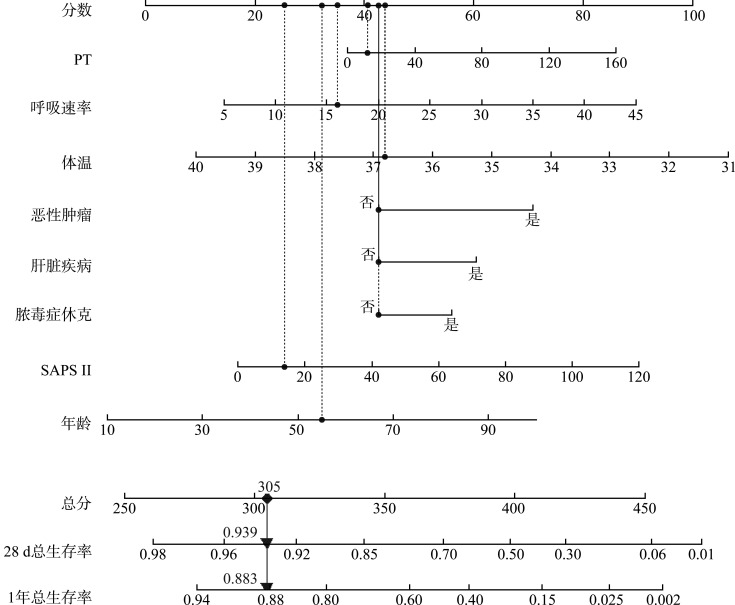
Results: A total of 14 240 patients with sepsis were included in our study. The 28-day and 1-year mortality were 21.45% (3 054 cases) and 36.50% (5 198 cases), respectively. Advanced age, female, high sepsis-related organ failure assessment (SOFA) score, high simplified acute physiology score II (SAPS II), rapid heart rate, rapid respiratory rate, septic shock, congestive heart failure, chronic obstructive pulmonary disease, liver disease, kidney disease, diabetes, malignant tumor, high white blood cell count (WBC), long prothrombin time (PT), and high serum creatinine (SCr) levels were all risk factors for sepsis death (all P<0.05). Eight variables, including PT, respiratory rate, body temperature, malignant tumor, liver disease, septic shock, SAPS II, and age were used to construct the model. The AUCs for 28-day and 1-year survival were 0.717 (95% CI 0.710 to 0.724) and 0.716 (95% CI 0.707 to 0.725), respectively. The calibration curve and decision curve showed that the model had good calibration degree and clinical application value.
Conclusions: The short-term and long-term mortality risk prediction models of patients with sepsis based on the MIMIC-IV database have good recognition ability and certain clinical reference significance for prognostic risk assessment and intervention treatment of patients.
目的: 鉴于脓毒症的高发病率和高病死率,早期识别高风险患者并及时干预至关重要,而现有死亡风险预测模型在操作、适用性和预测长期预后等方面均存在不足。本研究旨在探讨脓毒症患者死亡的危险因素,构建近期和远期死亡风险预测模型。方法: 从美国重症监护医学信息数据库IV(Medical Information Mart for Intensive Care-IV,MIMIC-IV)中选取符合脓毒症3.0诊断标准的人群,按7꞉3的比例随机分为建模组和验证组,分析患者的基线资料。采用单因素Cox回归分析和全子集回归确定脓毒症患者死亡的危险因素并筛选出构建预测模型的变量。分别用时间依赖性曲线下面积(area under the curve,AUC)、校准曲线和决策曲线评估模型的区分度、校准度和临床实用性。结果: 共纳入14 240例脓毒症患者,28 d和1年病死率分别为21.45%(3 054例)和36.50%(5 198例)。高龄、女性、高感染相关器官衰竭评分(sepsis-related organ failure assessment,SOFA)、高简明急性生理学评分(simplified acute physiology score II,SAPS II)、心率快、呼吸频率快、脓毒症休克、充血性心力衰竭、慢性阻塞性肺疾病、肝脏疾病、肾脏疾病、糖尿病、恶性肿瘤、高白细胞计数(white blood cell count,WBC)、长凝血酶原时间(prothrombin time,PT)、高血肌酐(serum creatinine,SCr)水平均为脓毒症死亡的危险因素(均P<0.05)。由PT、呼吸频率、体温、合并恶性肿瘤、合并肝脏疾病、脓毒症休克、SAPS II及年龄8个变量构建的模型,其28 d和1年生存的AUC分别为0.717(95% CI 0.710~0.724)和0.716(95% CI 0.707~0.725)。校准曲线和决策曲线表明该模型具有良好的校准度及较好的临床应用价值。结论: 基于MIMIC-IV建立的脓毒症患者近期和远期死亡风险预测模型有较好的识别能力,对患者预后风险评估及干预治疗具有一定的临床参考意义。.
Keywords: Medical Information Mart for Intensive Care-IV database; predictive model; prognostic factors; sepsis; short-term and long-term deaths.
Conflict of interest statement
作者声称无任何利益冲突。
Figures
Similar articles
-
[Development and validation of a prognostic model for patients with sepsis in intensive care unit].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023 Aug;35(8):800-806. doi: 10.3760/cma.j.cn121430-20230103-00003. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023. PMID: 37593856 Chinese.
-
[Constructing a predictive model for the death risk of patients with septic shock based on supervised machine learning algorithms].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024 Apr;36(4):345-352. doi: 10.3760/cma.j.cn121430-20230930-00832. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2024. PMID: 38813626 Chinese.
-
[Development and validation of a nomogram prediction model for in-hospital mortality risk in patients with sepsis complicated with acute pulmonary embolism].Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2025 Feb;37(2):123-127. doi: 10.3760/cma.j.cn121430-20240918-00778. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2025. PMID: 40017358 Chinese.
-
Prognostic factors and models to predict pediatric sepsis mortality: A scoping review.Front Pediatr. 2023 Feb 23;10:1022110. doi: 10.3389/fped.2022.1022110. eCollection 2022. Front Pediatr. 2023. PMID: 36908280 Free PMC article.
-
Mortality Prediction in the ICU.2016 Sep 10. In: MIT Critical Data, editor. Secondary Analysis of Electronic Health Records [Internet]. Cham (CH): Springer; 2016. Chapter 21. 2016 Sep 10. In: MIT Critical Data, editor. Secondary Analysis of Electronic Health Records [Internet]. Cham (CH): Springer; 2016. Chapter 21. PMID: 31314254 Free Books & Documents. Review.
Cited by
-
Artificial Intelligence-Assisted Clinical Decision-Making: A Perspective on Advancing Personalized Precision Medicine for Elderly Diabetes Patients.J Multidiscip Healthc. 2025 Aug 4;18:4643-4651. doi: 10.2147/JMDH.S529190. eCollection 2025. J Multidiscip Healthc. 2025. PMID: 40787142 Free PMC article.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
