

Immune-monitoring of myelodysplastic neoplasms: Recommendations from the i4MDS consortium
- PMID: 38756352
- PMCID: PMC11096644
- DOI: 10.1002/hem3.64
Immune-monitoring of myelodysplastic neoplasms: Recommendations from the i4MDS consortium
Abstract
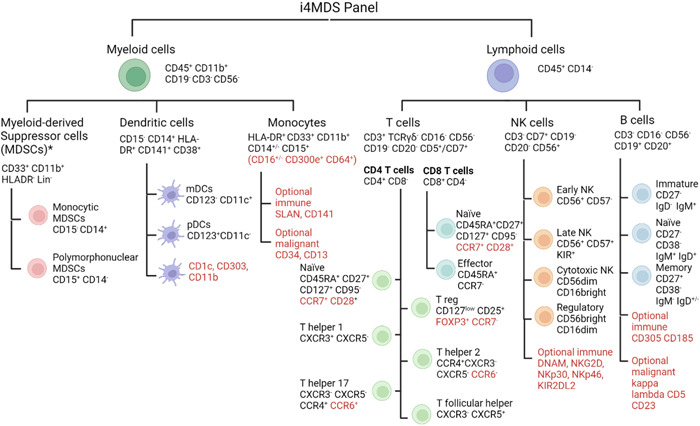
Advancements in comprehending myelodysplastic neoplasms (MDS) have unfolded significantly in recent years, elucidating a myriad of cellular and molecular underpinnings integral to disease progression. While molecular inclusions into prognostic models have substantively advanced risk stratification, recent revelations have emphasized the pivotal role of immune dysregulation within the bone marrow milieu during MDS evolution. Nonetheless, immunotherapy for MDS has not experienced breakthroughs seen in other malignancies, partly attributable to the absence of an immune classification that could stratify patients toward optimally targeted immunotherapeutic approaches. A pivotal obstacle to establishing "immune classes" among MDS patients is the absence of validated accepted immune panels suitable for routine application in clinical laboratories. In response, we formed International Integrative Innovative Immunology for MDS (i4MDS), a consortium of multidisciplinary experts, and created the following recommendations for standardized methodologies to monitor immune responses in MDS. A central goal of i4MDS is the development of an immune score that could be incorporated into current clinical risk stratification models. This position paper first consolidates current knowledge on MDS immunology. Subsequently, in collaboration with clinical and laboratory specialists, we introduce flow cytometry panels and cytokine assays, meticulously devised for clinical laboratories, aiming to monitor the immune status of MDS patients, evaluating both immune fitness and identifying potential immune "risk factors." By amalgamating this immunological characterization data and molecular data, we aim to enhance patient stratification, identify predictive markers for treatment responsiveness, and accelerate the development of systems immunology tools and innovative immunotherapies.
© 2024 The Authors. HemaSphere published by John Wiley & Sons Ltd on behalf of European Hematology Association.
Conflict of interest statement
Shahram Kordasti: Novartis: Advisory Board, Speakers bureau, Alexion: Speakers bureau, Beckman Coulter: Speakers bureau, MorphoSys: Research Support (none is related to this publication). Wolfgang Kern declares part‐ownership of MLL Munich Leukemia Laboratory. Austin Kulasekararaj: Research support (to institution): Celgene/BMS and Novartis. Speaker's fees: Alexion/AstraZeneca, Akari, Apellis, Celgene/BMS, Novartis, Pfizer, Ra Pharma/UCB, Roche, SOBI. Scientific advisory board: Alexion/Astra Zeneca, Apellis, Amgen, Agios, Biocryst, Celgene/BMS, Novartis, Pfizer, Regeneron, Roche, SOBI, Janssen, Samsung and Novo Nordisk (none is related to this publication).
Figures
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous