

V6 vein-preserving superior segmentectomy: A potentially preferable option
- PMID: 38756558
- PMCID: PMC11096962
- DOI: 10.1016/j.heliyon.2024.e30753
V6 vein-preserving superior segmentectomy: A potentially preferable option
Abstract
Objective: The increasing identification of pulmonary nodules has led to a growing emphasis on segmentectomy. Nevertheless, the surgical process for segmentectomy is complex and optimizing segmentectomy is a critical clinical concern. This study aimed to evaluate the safety and short- and long-term efficacy of V6-preserving superior segmentectomy.
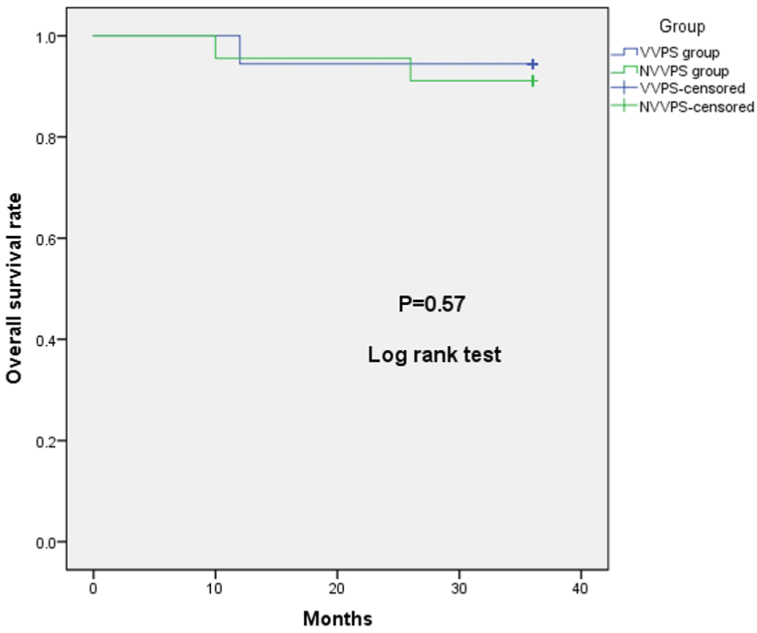
Methods: We performed a retrospective analysis of patients who underwent thoracoscopic superior segmentectomy at our hospital between January 2019 and June 2020. Eligible patients were categorized into an V6 vein-preserving segmentectomy (VVPS) group and a Non V6 vein-preserving segmentectomy (NVVPS) group depending on the preservation of V6. Primary outcome measures encompassed the evaluation of surgical safety (surgical margins, 3-year overall survival, and disease-free survival), whereas secondary measures included postoperative complication rates, operative time, estimated intraoperative blood loss, length of hospital stay, and associated costs.
Results: The analysis included a final cohort of 78 patients. In the NVVPS group (n = 43), 95.3 % of patients exceeded the tumor diameter, and no positive surgical margins were observed. The 3-year overall survival (OS) and disease-free survival (DFS) rates for the NVVPS group were 95.3 %, with no significant differences in OS (p = 0.572) and DFS (P = 0.800) compared with the VVPS group. Additionally, the median total hospitalization cost for the NVVPS group was 41,400 RMB (IQR, 38,800-43,400), which was significantly lower than that of the VVPS group, showing statistical significance (P < 0.05). No statistically significant differences were observed in the incidence of postoperative complications and length of stay between the two groups (P > 0.05).
Conclusion: V6-preserving superior segmentectomy is a secure and optimized surgical alternative. Its streamlined procedure facilitates easier adoption in primary healthcare facilities, rendering it a superior choice for superior segmentectomy.
Keywords: Pulmonary nodules; Segmental veins; Segmentectomy.
© 2024 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures


References
-
- Ginsberg R.J., Rubinstein L.V. Randomized trial of lobectomy versus limited resection for T1 N0 non-small cell lung cancer. Lung Cancer Study Group. Ann. Thorac. Surg. 1995 Sep;60(3):615–622. discussion 622-3. - PubMed
-
- Saji H., Okada M., Tsuboi M., et al. West Japan Oncology Group and Japan Clinical Oncology Group. Segmentectomy versus lobectomy in small-sized peripheral non-small-cell lung cancer (JCOG0802/WJOG4607L): a multicentre, open-label, phase 3, randomised, controlled, non-inferiority trial. Lancet. 2022 Apr 23;399(10335):1607–1617. - PubMed
-
- Suzuki K., Saji H., Aokage K., et al. West Japan oncology group; Japan clinical oncology group. Comparison of pulmonary segmentectomy and lobectomy: safety results of a randomized trial. J. Thorac. Cardiovasc. Surg. 2019 Sep;158(3):895–907. - PubMed
LinkOut - more resources
Full Text Sources
