

Differences in Patterns of Care and Referral Between Proton and Photon Therapy
- PMID: 38757072
- PMCID: PMC11095099
- DOI: 10.1016/j.ijpt.2023.10.001
Differences in Patterns of Care and Referral Between Proton and Photon Therapy
Abstract
Purpose: To report demographic and clinical characteristics of patients who were more likely to receive proton beam therapy (PBT) than photon therapy from facilities with access to proton centers.
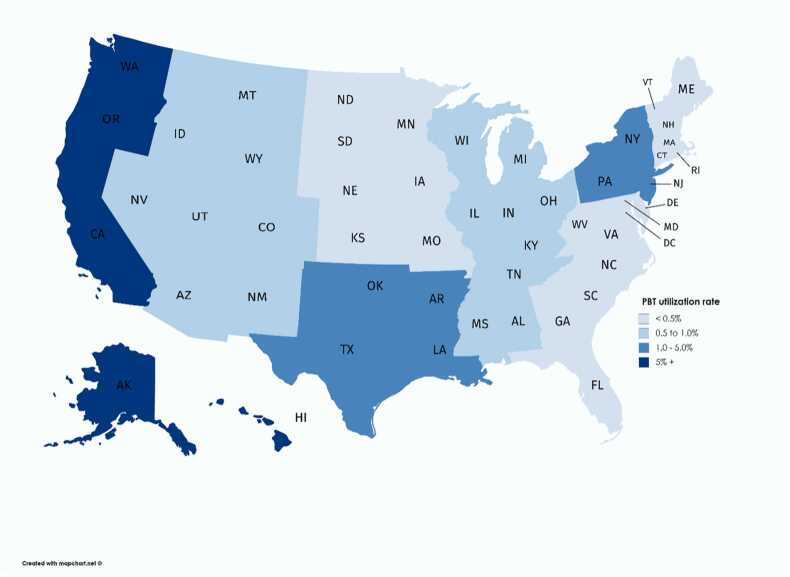
Materials and methods: We utilized the national cancer database to identify the facilities with access to PBT between 2004 and 2015 and compared the relative usage of photons and PBT for demographic and clinical scenarios in breast, prostate, and nonsmall cell cancer.
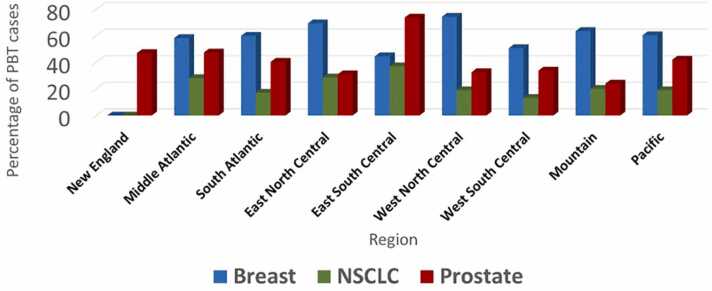
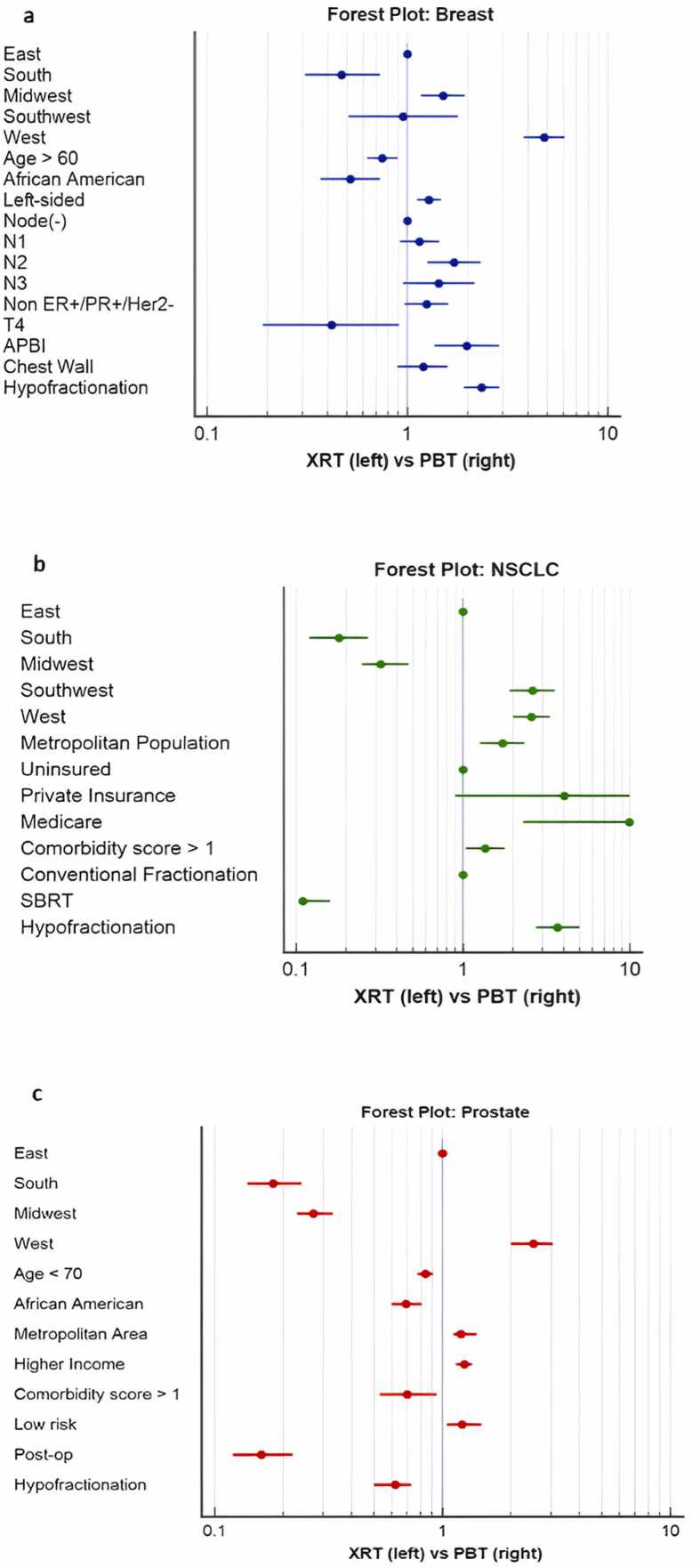
Results: In total, 231 facilities with access to proton centers accounted for 168 323 breast, 39 975 lung, and 77 297 prostate cancer patients treated definitively. Proton beam therapy was used in 0.5%, 1.5%, and 8.9% of breast, lung, and prostate cases. Proton beam therapy was correlated with a farther distance traveled and longer start time from diagnosis for each site (P < .05).For breast, demographic correlates of PBT were treatment in the west coast (odds ratio [OR] = 4.81), age <60 (OR = 1.25), white race (OR = 1.94), and metropolitan area (OR = 1.58). Left-sided cancers (OR = 1.28), N2 (OR = 1.71), non-ER+/PR+/Her2Neu- cancers (OR = 1.24), accelerated partial breast irradiation (OR = 1.98), and hypofractionation (OR = 2.35) were predictors of PBT.For nonsmall cell cancer, demographic correlates of PBT were treatment in the south (OR = 2.6), metropolitan area (OR = 1.72), and Medicare insurance (OR = 1.64). Higher comorbid score (OR = 1.36), later year treated (OR = 3.16), and hypofractionation (not SBRT) (OR = 3.7) were predictors of PBT.For prostate, correlates of PBT were treatment in the west coast (OR = 2.48), age <70 (OR = 1.19), white race (OR = 1.41), metropolitan area (OR = 1.25), higher income/education (OR = 1.25), and treatment at an academic center (OR = 33.94). Lower comorbidity score (OR = 1.42), later year treated (OR = 1.37), low-risk disease (OR = 1.45), definitive compared to postoperative (OR = 6.10), and conventional fractionation (OR = 1.64) were predictors of PBT.
Conclusion: Even for facilities with established referrals to proton centers, PBT utilization was low; socioeconomic status was potentially a factor. Proton beam therapy was more often used with left-sided breast and low-risk prostate cancers, without a clear clinical pattern in lung cancer.
Keywords: Disparities; Proton centers; Referral patterns.
© 2024 The Authors.
Conflict of interest statement
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Figures
Similar articles
-
Patient characterization and usage trends of proton beam therapy for localized prostate cancer in the United States: A study of the National Cancer Database.Urol Oncol. 2017 Jun;35(6):438-446. doi: 10.1016/j.urolonc.2017.01.013. Epub 2017 Feb 15. Urol Oncol. 2017. PMID: 28214281
-
Association of Race With Receipt of Proton Beam Therapy for Patients With Newly Diagnosed Cancer in the US, 2004-2018.JAMA Netw Open. 2022 Apr 1;5(4):e228970. doi: 10.1001/jamanetworkopen.2022.8970. JAMA Netw Open. 2022. PMID: 35471569 Free PMC article.
-
Proton beam therapy versus stereotactic body radiotherapy for hepatocellular carcinoma: practice patterns, outcomes, and the effect of biologically effective dose escalation.J Gastrointest Oncol. 2019 Oct;10(5):999-1009. doi: 10.21037/jgo.2019.08.03. J Gastrointest Oncol. 2019. PMID: 31602338 Free PMC article.
-
Health Disparities and Inequities in the Utilization of Proton Therapy for Prostate Cancer.Cancers (Basel). 2024 Nov 15;16(22):3837. doi: 10.3390/cancers16223837. Cancers (Basel). 2024. PMID: 39594791 Free PMC article. Review.
-
A Literature Review of Proton Beam Therapy for Prostate Cancer in Japan.J Clin Med. 2019 Jan 5;8(1):48. doi: 10.3390/jcm8010048. J Clin Med. 2019. PMID: 30621278 Free PMC article. Review.
Cited by
-
Utilizing proton therapy to reduce health-care disparities among patients with breast cancers.JNCI Cancer Spectr. 2025 Jan 3;9(1):pkaf003. doi: 10.1093/jncics/pkaf003. JNCI Cancer Spectr. 2025. PMID: 39996603 Free PMC article. No abstract available.
References
LinkOut - more resources
Full Text Sources
Research Materials