

PTCOG Gastrointestinal Subcommittee Lower Gastrointestinal Tract Malignancies Consensus Statement
- PMID: 38757077
- PMCID: PMC11095104
- DOI: 10.1016/j.ijpt.2024.100019
PTCOG Gastrointestinal Subcommittee Lower Gastrointestinal Tract Malignancies Consensus Statement
Abstract
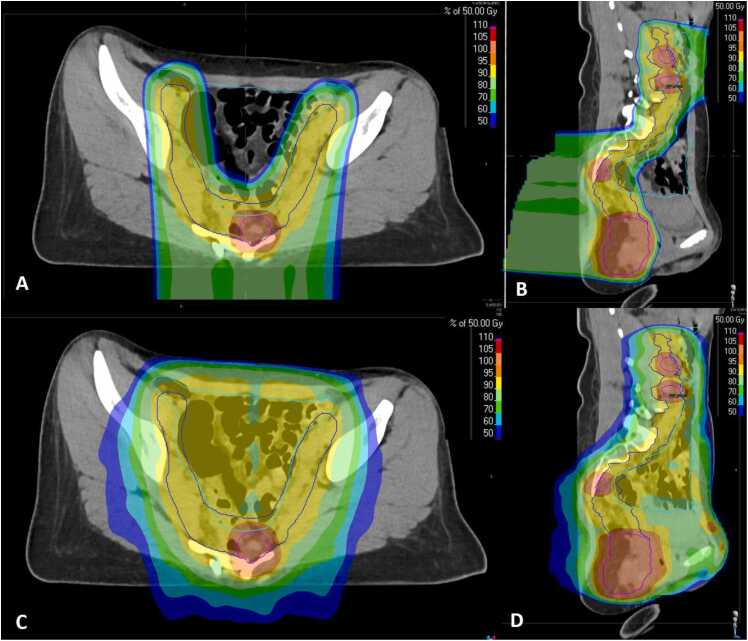
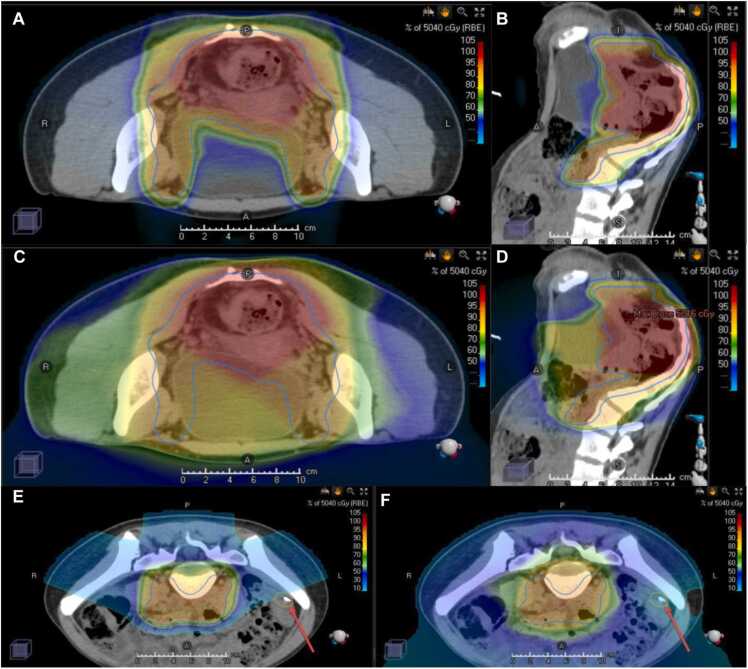
Purpose: Radiotherapy delivery in the definitive management of lower gastrointestinal (LGI) tract malignancies is associated with substantial risk of acute and late gastrointestinal (GI), genitourinary, dermatologic, and hematologic toxicities. Advanced radiation therapy techniques such as proton beam therapy (PBT) offer optimal dosimetric sparing of critical organs at risk, achieving a more favorable therapeutic ratio compared with photon therapy.
Materials and methods: The international Particle Therapy Cooperative Group GI Subcommittee conducted a systematic literature review, from which consensus recommendations were developed on the application of PBT for LGI malignancies.
Results: Eleven recommendations on clinical indications for which PBT should be considered are presented with supporting literature, and each recommendation was assessed for level of evidence and strength of recommendation. Detailed technical guidelines pertaining to simulation, treatment planning and delivery, and image guidance are also provided.
Conclusion: PBT may be of significant value in select patients with LGI malignancies. Additional clinical data are needed to further elucidate the potential benefits of PBT for patients with anal cancer and rectal cancer.
Keywords: Anal cancer; Proton therapy; Quality of life; Rectal cancer; Toxicity.
© 2024 The Authors.
Figures


References
-
- Siegel R.L., Miller K.D., Wagle N.S., Jemal A. Cancer statistics, 2023. CA Cancer J Clin. 2023;73(1):17–48. - PubMed
-
- Sauer R., Becker H., Hohenberger W., et al. Preoperative versus postoperative chemoradiation therapy for rectal cancer. N Engl J Med. 2004;351:1731–1740. - PubMed
-
- Valentini V., Morganti A.G., Gambacorta M.A., et al. Preoperative hyperfractionated chemoradiation for locally recurrent rectal cancer in patients previously irradiated to the pelvis: a multicentric phase II study. Int J Radiat Oncol Biol Phys. 2006;64(4):1129–1139. - PubMed
-
- Gerard J., Conroy T., Bonnetain F., et al. Preoperative radiotherapy with or without concurrent fluorouracil and leucovorin in T3-4 rectal cancers: results of FFCD 9203. J Clin Onc. 2006;24(28):4620–4625. - PubMed
-
- UKCCCR Anal Cancer Trial Working Party Epidermoid anal cancer: results from the UKCCCR randomized trial of radiotherapy alone versus radiotherapy, 5-fluorouracil, and mitomycin. Lancet. 1996;348(9034):1049–1054. - PubMed
Publication types
LinkOut - more resources
Full Text Sources