

The causal relationship between sarcopenia-related traits and ischemic stroke: Insights from univariable and multivariable Mendelian randomization analyses
- PMID: 38757378
- PMCID: PMC11099748
- DOI: 10.1111/cns.14759
The causal relationship between sarcopenia-related traits and ischemic stroke: Insights from univariable and multivariable Mendelian randomization analyses
Abstract
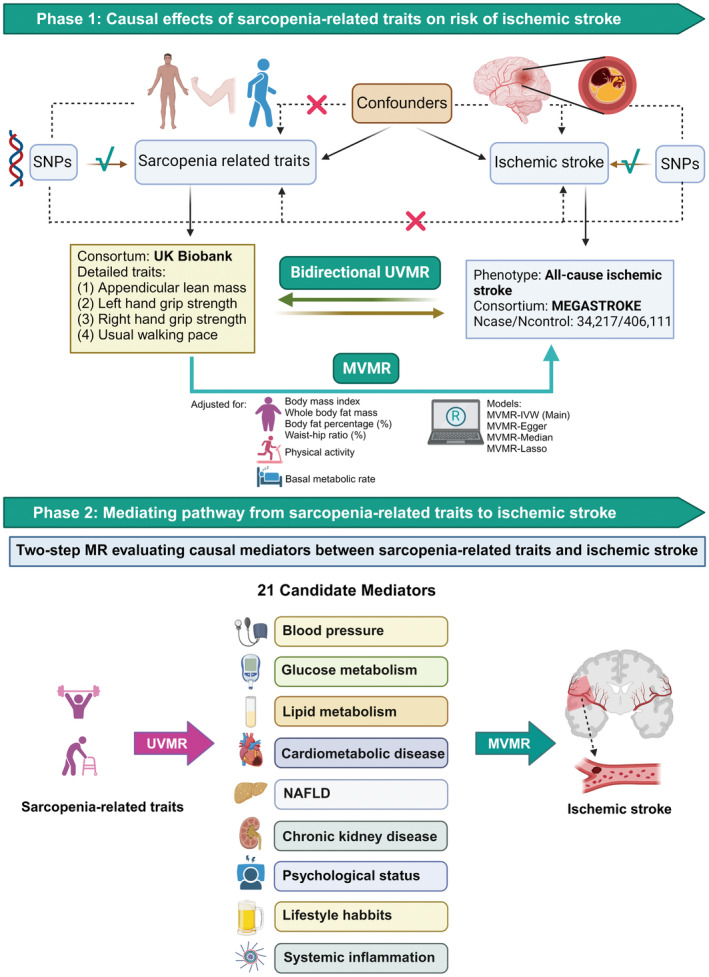
Aims: The causal relationship between sarcopenia-related traits and ischemic stroke (IS) remains poorly understood. This study aimed to explore the causal impact of sarcopenia-related traits on IS and to identify key mediators of this association.
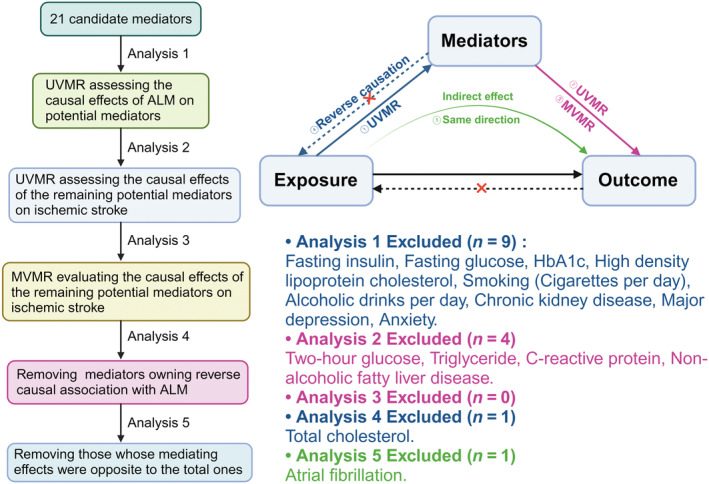
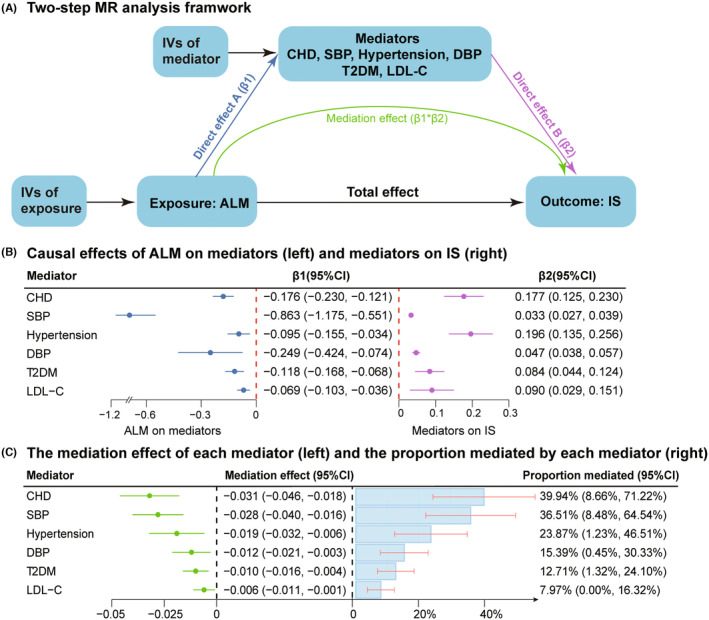
Methods: We conducted univariable, multivariable two-sample, and two-step Mendelian randomization (MR) analyses using genome-wide association study (GWAS) data. This included data for appendicular lean mass (ALM), hand grip strength (HGS), and usual walking pace (UWP) from the UK Biobank, and IS data from the MEGASTROKE consortium. Additionally, 21 candidate mediators were analyzed based on their respective GWAS data sets.
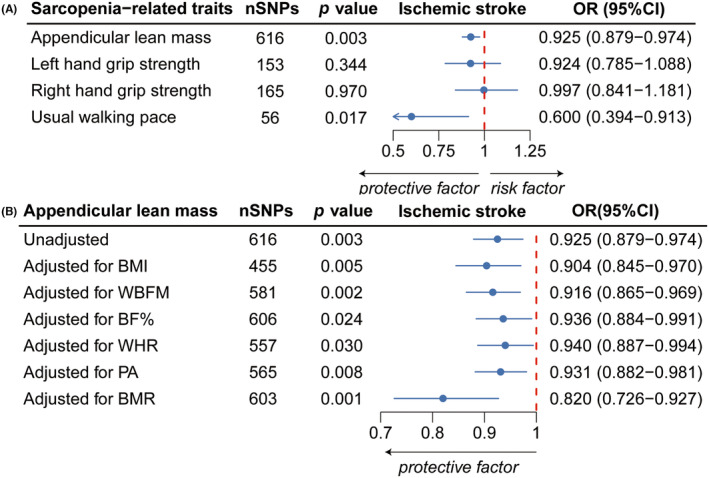
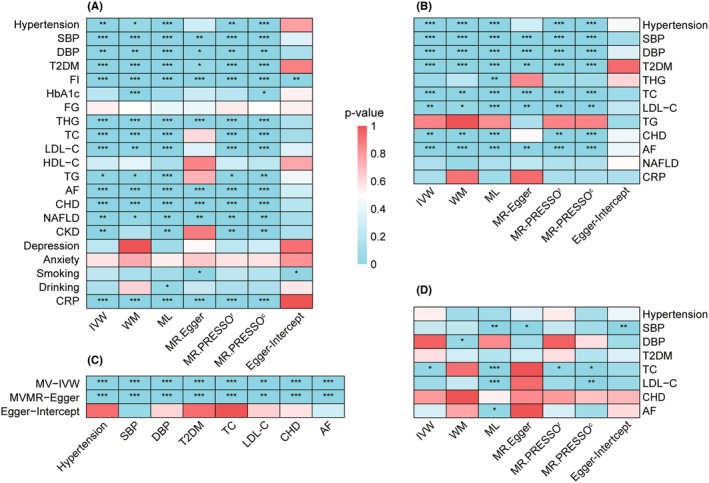
Results: Each 1-SD increase in genetically proxied ALM was associated with a 7.5% reduction in the risk of IS (95% CI: 0.879-0.974), and this correlation remained after controlling for levels of physical activity and adiposity-related indices. Two-step MR identified that six mediators partially mediated the protective effect of higher ALM on IS, with the most significant being coronary heart disease (CHD, mediating proportion: 39.94%), followed by systolic blood pressure (36.51%), hypertension (23.87%), diastolic blood pressure (15.39%), type-2 diabetes mellitus (T2DM, 12.71%), and low-density lipoprotein cholesterol (7.97%).
Conclusion: Our study revealed a causal protective effect of higher ALM on IS, independent of physical activity and adiposity-related indices. Moreover, we found that higher ALM could reduce susceptibility to IS partially by lowering the risk of vascular risk factors, including CHD, hypertension, T2DM, and hyperlipidemia. In brief, we elucidated another modifiable factor for IS and implied that maintaining sufficient muscle mass may reduce the risk of such disease.
Keywords: Mendelian randomization; appendicular lean mass; ischemic stroke; mediators; sarcopenia.
© 2024 The Authors. CNS Neuroscience & Therapeutics published by John Wiley & Sons Ltd.
Conflict of interest statement
It is noteworthy that this study only used publicly available summary‐level GWAS data and did not involve the utilization of individual‐level statistics, thus no ethical approval was required. No potential conflict of interest was reported by the authors.
Figures
References
-
- Pu L, Wang L, Zhang R, Zhao T, Jiang Y, Han L. Projected global trends in ischemic stroke incidence, deaths and disability‐adjusted life years from 2020 to 2030. Stroke. 2023;54(5):1330‐1339. - PubMed
-
- Saini V, Guada L, Yavagal DR. Global epidemiology of stroke and access to acute ischemic stroke interventions. Neurology. 2021;97(20 Suppl 2):S6‐s16. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
