

Safety and clinical outcomes of endovascular therapy versus medical management in late presentation of large ischemic stroke
- PMID: 38757713
- PMCID: PMC11569454
- DOI: 10.1177/23969873241249406
Safety and clinical outcomes of endovascular therapy versus medical management in late presentation of large ischemic stroke
Abstract
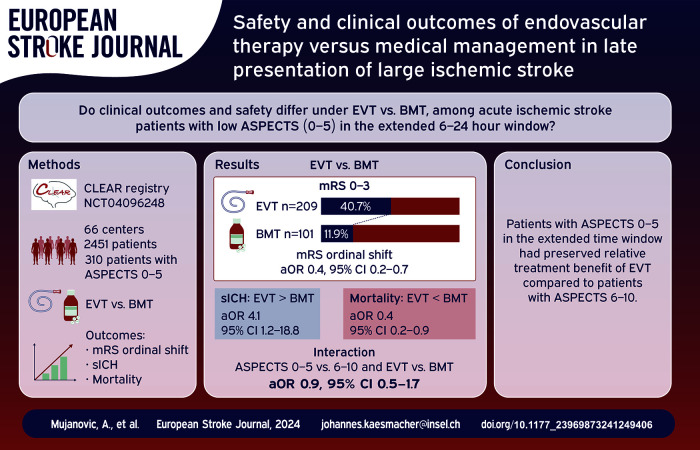
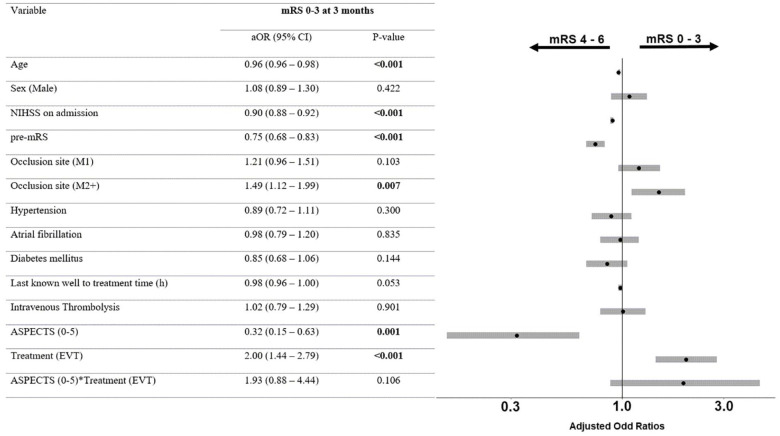
Introduction: The benefit of endovascular therapy (EVT) among stroke patients with large ischemic core (ASPECTS 0-5) in the extended time window outside of trial settings remains unclear. We analyzed the effect of EVT among these stroke patients in real-world settings.
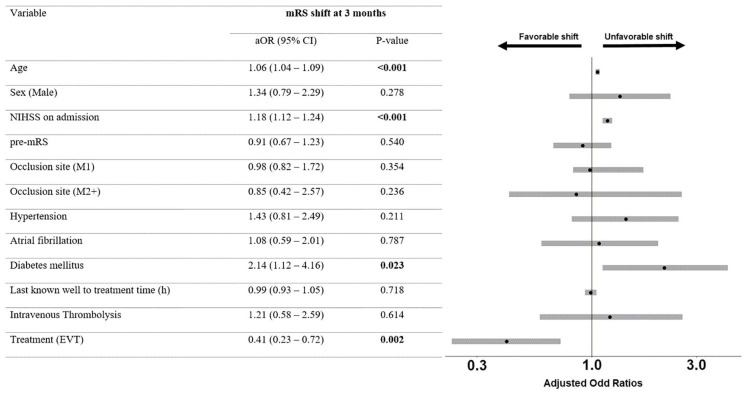
Patients and methods: The CT for Late Endovascular Reperfusion (CLEAR) study recruited patients from 66 centers in 10 countries between 01/2014 and 05/2022. The extended time-window was defined as 6-24 h from last-seen-well to treatment. The primary outcome was shift of the 3-month modified Rankin scale (mRS) score. Safety outcomes included symptomatic intracranial hemorrhage (sICH) and mortality. Outcomes were analyzed with ordinal and logistic regressions.
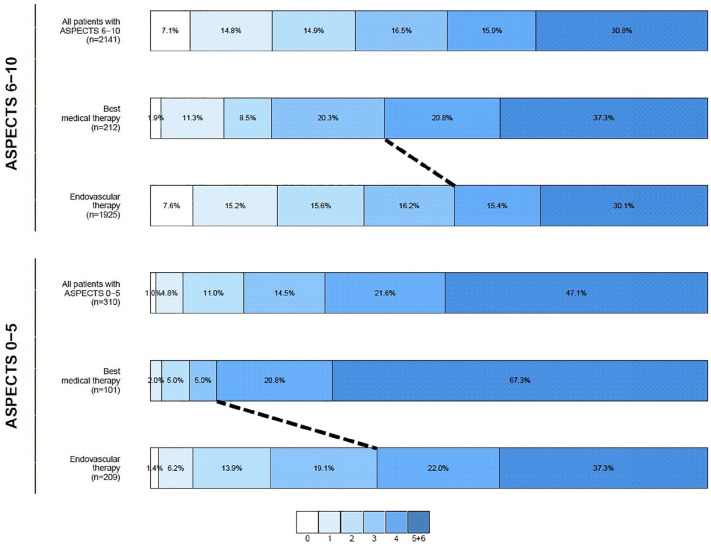
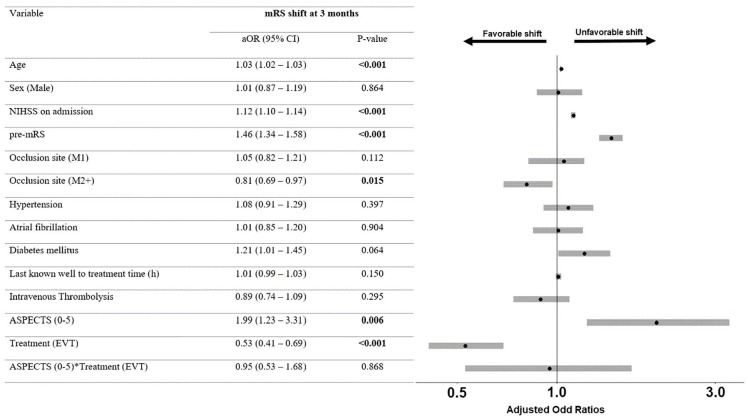
Results: Among 5098 screened patients, 2451 were included in the analysis (median age 73, 55% women). Of patients with ASPECTS 0-5 (n = 310), receiving EVT (n = 209/310) was associated with lower 3-month mRS when compared to medical management (median 4 IQR 3-6 vs 6 IQR 4-6; aOR 0.4, 95% CI 0.2-0.7). Patients undergoing EVT had higher sICH (11.2% vs 4.0%; aOR 4.1, 95% CI 1.2-18.8) and lower mortality (31.6% vs 58.4%, aOR 0.4; 95% CI 0.2-0.9) compared to medically managed patients. The relative benefit of EVT was comparable between patients with ASPECTS 0 and 5 and 6-10 in the extended time window (interaction aOR 0.9; 95% CI 0.5-1.7).
Conclusion: In the extended time window, patients with ASPECTS 0-5 may have preserved relative treatment benefit of EVT compared to patients with ASPECTS 6-10. These findings are in line with recent trials showing benefit of EVT among real-world patients with large ischemic core in the extended time window.
Trial registration number: clinicaltrials.gov; Unique identifier: NCT04096248.
Keywords: Endovascular therapy; best medical treatment; extended time-window; large ischemic core; mechanical thrombectomy.
Conflict of interest statement
Declaration of conflicting interestsThe author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: U.Fischer reported research support of the Swiss National Science Foundation and the Swiss Heart Foundation; research grants from Medtronic (BEYOND SWIFT, SWIFT DIRECT) and from Stryker, Rapid medical, Penumbra and Phenox (DISTAL); consultancies for Medtronic, Stryker, and CSL Behring; participation in an advisory board for Alexion/Portola, Boehringer Ingelheim, Biogen and Acthera; member of a clinical event committee (CEC) of the COATING study (Phenox) and member of the data and safety monitoring committee (DSMB) of the TITAN, LATE_MT and IN EXTREMIS trials; presidency of the Swiss Neurological Society. All fees are paid to institutions. T.Dobrocky reported MicroVention consultancy. H.Henon reported grants from SANOFI-AVENTIS U.S. LLC. D.Haussen reported consultancy for Vesalio, Cerenovus, Stryker, Brainomix, Poseydon Medical, and Chiesi USA; DSMB from Jacobs Institute; stock options in Viz AI. J.Kaesmacher reported grants from Swiss Academy of Medical Sciences/Bangerter Foundation, Swiss Stroke Society, Clinical Trials Unit Bern. J. Siegler reported grants from Medtronic and Philips. D.Kaiser reported grants from Joachim Herz Foundation. N.Martinez-Majander reported grants from Finnish Medical Foundation. J.P.Marto reported consulting and speaker fees from Amicus Therapeutics and Boehringer Ingelheim. P.Michel reported grants from University of Lausanne, Swiss National Science Foundation. M.Möhlenbruch reported grants from Medtronic, Stryker, MicroVention. S.Nagel reported consultancy for Brainomix; speaker Boehringer Ingelheim, Pfizer. T.Nguyen discloses research support from Medtronic to her institution; advisory board Idorsia, Brainomix, ArunaBio; Associate Editor of Stroke. R.Nogueira reported consultancy for Biogen, Brainomix, Corindus, Cerenovus, Stryker, Medtronic, Ceretrieve, Anaconda, Biomed, Vesalio, Imperative Care, NeuroVasc Technologies, Viz AI, Genentech, Prolong Pharmaceuticals, Perfuze, Phenox, RapidPulse; stock options Viz AI, Vesalio, Perfuze, Corindus, Brainomix, Ceretrieve; grants from Cerenovus, Stryker. V.Puetz reported lecturer fee for Daiichi Sankyo. M.Ribo reported consultancy for Medtronic, MiniMed, Cerenovus, AptaTargets, Stryker, Philips; stock holdings in Methinks, Nora, Anaconda Biomed. P.Ringleb reported travel support from Bayer, Bristol Myers Squibb; consultancy for Daiichi Sankyo Company, Boehringer Ingelheim. S.Sheth reported consultancy for Imperative Care, Viz AI, Penumbra, Motif Neurosciences; NIH grant. S. Yoshimura reported research grants from Medico’s Hirata, Medtronic, and Terumo; and lecturer fees from Medtronic, Kaneka, Stryker, Daiichi Sankyo, Bristol-Meyers Squibb, and Johnson & Johnson. Sakai reported a research grant from Japan Lifeline, Kaneka, Medtronic, Terumo and TG Medical; lecturer’s fees from Asahi-Intec, Kaneka, Medtronic, Stryker and Terumo; advisory boards for Johnson&Johnson, Medtronic and Terumo. H.Yamagami reported research grants from Bristol-Myers Squibb; lecturer’s fees from Stryker, Medtronic, J&J, Bayer, Daiichi Sankyo, Bristol-Myers Squibb, Otuska Pharmaceutical; advisory board for Daiichi Sankyo. D. Strbian reported research grant from the governmental educational funding (Finland), hospital research funds (HUS), unrestricted educational grant (Boehringer Ingelheim), whereas all funds were handled by hospital-based institution; partner of the consortium funding for the PROOF trial (EU), LVO check (EU), and electric impedance tomography project (Jane ja Aatos Erkon Säätiö); consultancies and advisory scientific board for Orion, Herantis Pharma, Boehringer Ingelheim, Portola, Alexion, AstraZeneca, Bristol-Meyers-Squibb, Janssen; member of the DSMB on the ENDOLOW trial. All other authors declare no conflict of interest.
Figures
References
-
- Powers W, Rabinstein A, Ackerson T, et al.. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke a guideline for healthcare professionals from the American Heart Association/American Stroke Association. 2019; 50: e344–e418. DOI: 10.1161/STR.0000000000000211. - DOI - PubMed
-
- Nguyen TN, Castonguay AC, Siegler JE, et al.. Mechanical thrombectomy in the late presentation of anterior circulation large vessel occlusion stroke: a guideline from the Society of Vascular and Interventional Neurology guidelines and practice standards committee. Stroke Vasc Interv Neurol 2023; 3: e000512. - PMC - PubMed
-
- Goyal M, Menon BK, van Zwam WH, et al.. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet 2016; 387: 1723–1731. - PubMed
-
- Yoshimura S, Sakai N, Yamagami H, et al.. Endovascular therapy for acute stroke with a large ischemic region. New Engl J Med 2022; 386: 1303–1313. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
