Pathophysiology, Diagnosis, Prognosis, and Prevention of Poststroke Epilepsy: Clinical and Research Implications
- PMID: 38759128
- PMCID: PMC11175639
- DOI: 10.1212/WNL.0000000000209450
Pathophysiology, Diagnosis, Prognosis, and Prevention of Poststroke Epilepsy: Clinical and Research Implications
Abstract
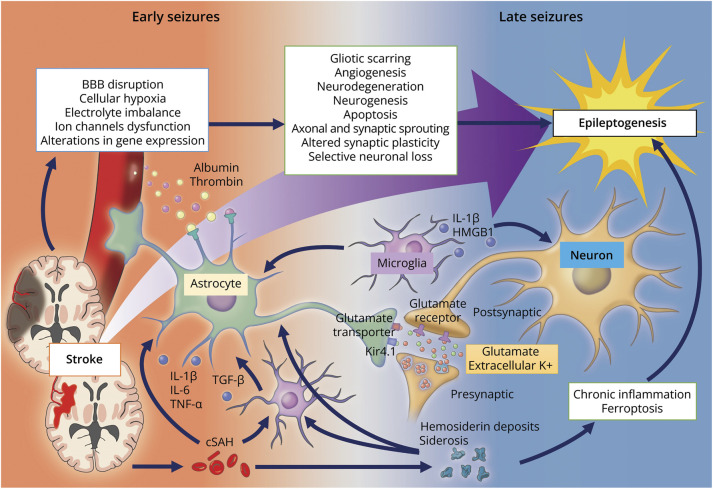
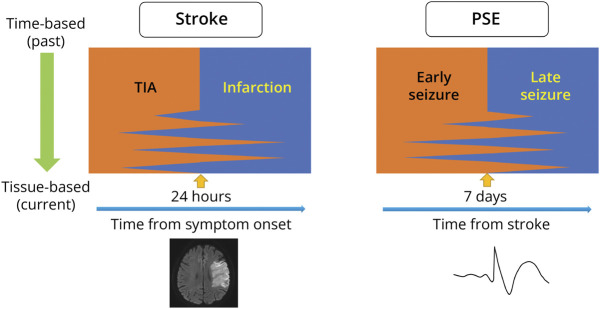
Poststroke epilepsy (PSE) is associated with higher mortality and poor functional and cognitive outcomes in patients with stroke. With the remarkable development of acute stroke treatment, there is a growing number of survivors with PSE. Although approximately 10% of patients with stroke develop PSE, given the significant burden of stroke worldwide, PSE is a significant problem in stroke survivors. Therefore, the attention of health policymakers and significant funding are required to promote PSE prevention research. The current PSE definition includes unprovoked seizures occurring more than 7 days after stroke onset, given the high recurrence risks of seizures. However, the pathologic cascade of stroke is not uniform, indicating the need for a tissue-based approach rather than a time-based one to distinguish early seizures from late seizures. EEG is a commonly used tool in the diagnostic work-up of PSE. EEG findings during the acute phase of stroke can potentially stratify the risk of subsequent seizures and predict the development of poststroke epileptogenesis. Recent reports suggest that cortical superficial siderosis, which may be involved in epileptogenesis, is a promising marker for PSE. By incorporating such markers, future risk-scoring models could guide treatment strategies, particularly for the primary prophylaxis of PSE. To date, drugs that prevent poststroke epileptogenesis are lacking. The primary challenge involves the substantial cost burden due to the difficulty of reliably enrolling patients who develop PSE. There is, therefore, a critical need to determine reliable biomarkers for PSE. The goal is to be able to use them for trial enrichment and as a surrogate outcome measure for epileptogenesis. Moreover, seizure prophylaxis is essential to prevent functional and cognitive decline in stroke survivors. Further elucidation of factors that contribute to poststroke epileptogenesis is eagerly awaited. Meanwhile, the regimen of antiseizure medications should be based on individual cardiovascular risk, psychosomatic comorbidities, and concomitant medications. This review summarizes the current understanding of poststroke epileptogenesis, its risks, prognostic models, prophylaxis, and strategies for secondary prevention of seizures and suggests strategies to advance research on PSE.
Conflict of interest statement
T. Tanaka, M. Ihara, K. Fukuma, and A. Guekht report no disclosures relevant to the manuscript. N.K. Mishra is a member of the editorial board of
Figures