

Combining inertial navigation with transacetabular ligament in total hip arthroplasty via direct anterior approach results in excellent accuracy compared to standard manual technique - A retrospective cohort study
- PMID: 38759152
- PMCID: PMC11101203
- DOI: 10.1051/sicotj/2024013
Combining inertial navigation with transacetabular ligament in total hip arthroplasty via direct anterior approach results in excellent accuracy compared to standard manual technique - A retrospective cohort study
Abstract
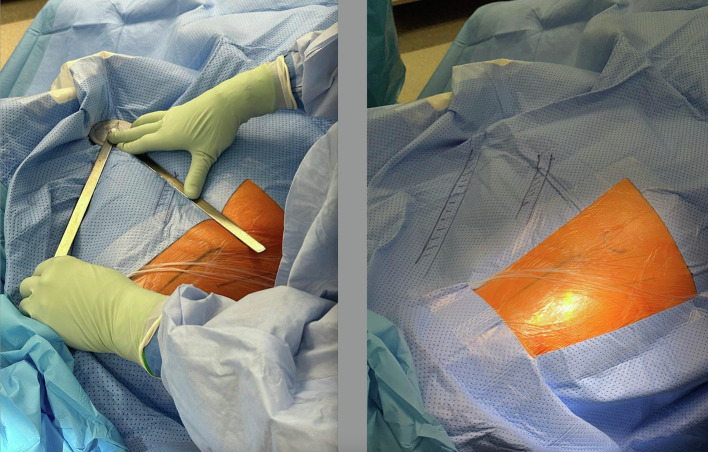
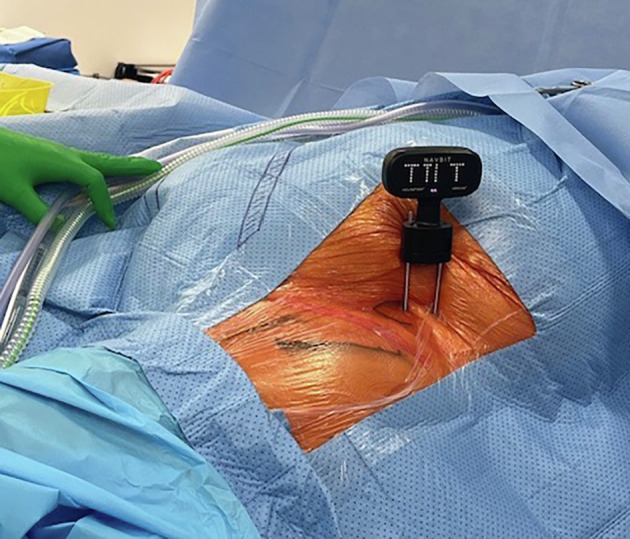
Background: Correct acetabular component placement plays a critical role in reducing early revisions after dislocations in total hip arthroplasty (THA). Although the transverse acetabular ligament (TAL) guides anteversion, inclination can only be accurately guided by navigation. In order to overcome the initial disadvantages with navigation, an imageless, easy-to-use inertial navigation system has been recently introduced. This study aims to analyze the accuracy of inclination with this navigation system compared to the standard manual technique.
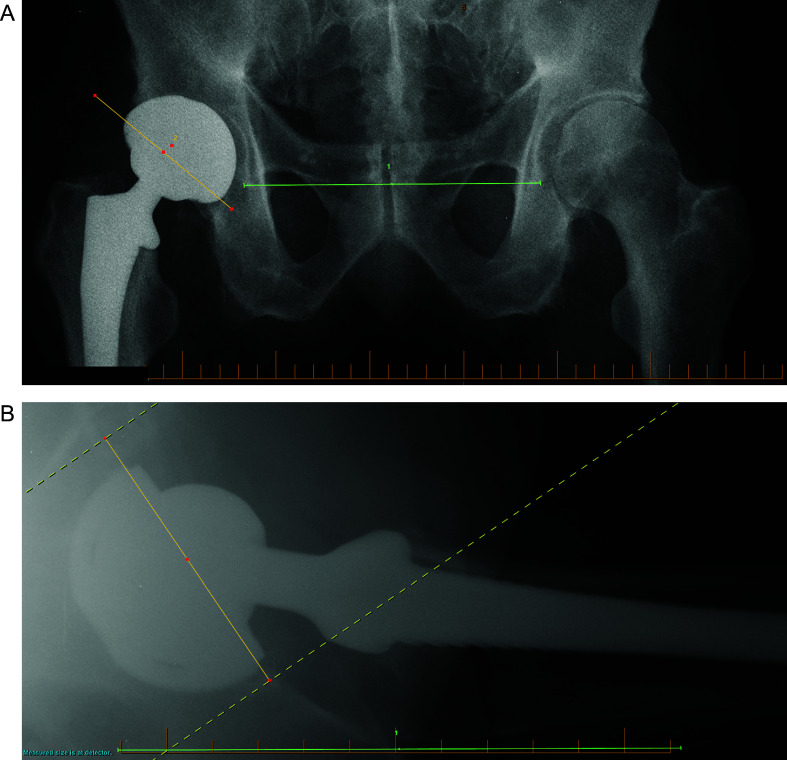
Methods: Two cohorts, manual technique (MT) and navigation (NAV) cohorts, consisted of 83 and 95 patients, respectively, after exclusion criteria were applied. Inclination target was 38° and anteversion was guided by TAL. Demographic data were collected, and anteroposterior (AP) pelvic and cross-table lateral radiographs were obtained 6 weeks post-operatively. Inclination and anteversion were determined on the AP pelvic and cross-table lateral radiograph, respectively.
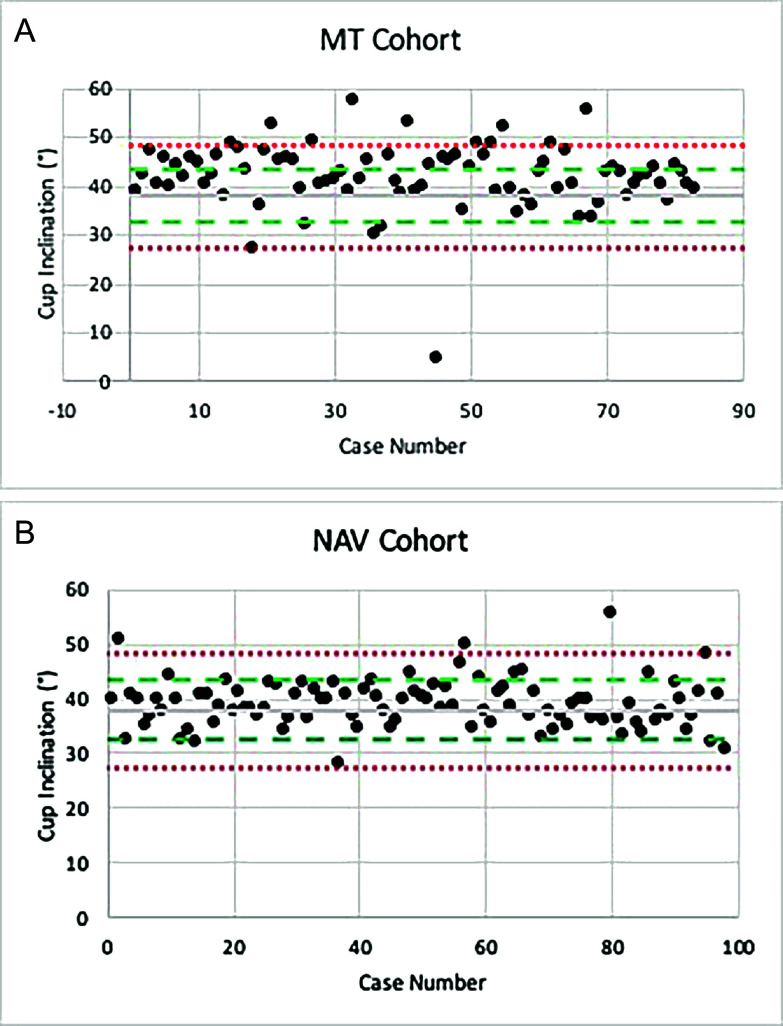
Results: A mean inclination of 41.8° (±6.8°) and 38.9° (±4.4°) was found in the MT and NAV cohorts, respectively. There was no statistical difference in gender, age, and BMI. If the inclination was set within 10° of the target (i.e., 38°), 88% of the MT cohort and 97% of the NAV cohort were within the target zone. Accuracy decreased to 53% and 83%, respectively, if the target zone range was narrowed down to ± 5°.
Conclusion: Combining inertial imageless navigation for inclination and TAL as a landmark for anteversion is significantly more accurate compared to the manual technique, without having the limitations and disadvantages of current standard navigational techniques.
Keywords: Navigation; Total hip arthroplasty; Transverse acetabular ligament.
© The Authors, published by EDP Sciences, 2024.
Conflict of interest statement
The authors declare that they have no relevant financial or non-financial interests to report.
Figures
Similar articles
-
Acetabular Component Positioning Using the Transverse Acetabular Ligament as an Anatomical Landmark in Primary Total Hip Arthroplasty: A Prospective Study.Cureus. 2025 Apr 9;17(4):e81940. doi: 10.7759/cureus.81940. eCollection 2025 Apr. Cureus. 2025. PMID: 40351948 Free PMC article.
-
Which one is more affected by navigation-assisted cup positioning in total hip arthroplasty: Anteversion or inclination? A retrospective matched-pair cohort study in Asian physique.J Orthop Surg (Hong Kong). 2018 May-Aug;26(2):2309499018780755. doi: 10.1177/2309499018780755. J Orthop Surg (Hong Kong). 2018. PMID: 29890935
-
Image-Less THA Cup Navigation in Clinical Routine Setup: Individual Adjustments, Accuracy, Precision, and Robustness.Medicina (Kaunas). 2022 Jun 20;58(6):832. doi: 10.3390/medicina58060832. Medicina (Kaunas). 2022. PMID: 35744095 Free PMC article.
-
Application of transverse acetabular ligament in total hip arthroplasty: a systematic review.BMC Musculoskelet Disord. 2023 Apr 13;24(1):284. doi: 10.1186/s12891-023-06410-0. BMC Musculoskelet Disord. 2023. PMID: 37055756 Free PMC article.
-
Imageless navigation versus traditional method in total hip arthroplasty: A meta-analysis.Int J Surg. 2015 Sep;21:122-7. doi: 10.1016/j.ijsu.2015.07.707. Epub 2015 Aug 5. Int J Surg. 2015. PMID: 26253850 Review.
Cited by
-
Effects of the Flip Technique on Measurement Accuracy of the Acetabular Cup Position Using a Portable Hip Navigation System With Patients in the Lateral Decubitus Position.Arthroplast Today. 2025 Jul 8;34:101769. doi: 10.1016/j.artd.2025.101769. eCollection 2025 Aug. Arthroplast Today. 2025. PMID: 40686660 Free PMC article.
References
-
- Australian Orthopaedic Association National Joint Replacement Registry (AOANJRR) (2022) Hip, knee & shoulder arthroplasty: 2022 annual report. AOA, Adelaide. Available at https://aoanjrr.sahmri.com/annual-reports-2022.
-
- Lewinnek GE, Lewis JL, Tarr R, Compere CL, Zimmerman JR (1978) Dislocations after total hip-replacement arthroplasties. J Bone Jt Surg Am 60, 217–220. - PubMed
-
- Wan Z, Boutary M, Dorr LD (2008) The influence of acetabular component position on wear in total hip arthroplasty. J Arthroplasty 23, 51–56. - PubMed
-
- Hevesi M, Wyles CC, Rouzrokh P, et al. (2022) Redefining the 3D topography of the acetabular safe zone. J Bone Jt Surg 104, 239–245. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous