

Comparison of HPV-positive triage strategies combining extended genotyping with cytology or p16/ki67 dual staining in the Italian NTCC2 study
- PMID: 38759278
- PMCID: PMC11126882
- DOI: 10.1016/j.ebiom.2024.105149
Comparison of HPV-positive triage strategies combining extended genotyping with cytology or p16/ki67 dual staining in the Italian NTCC2 study
Abstract
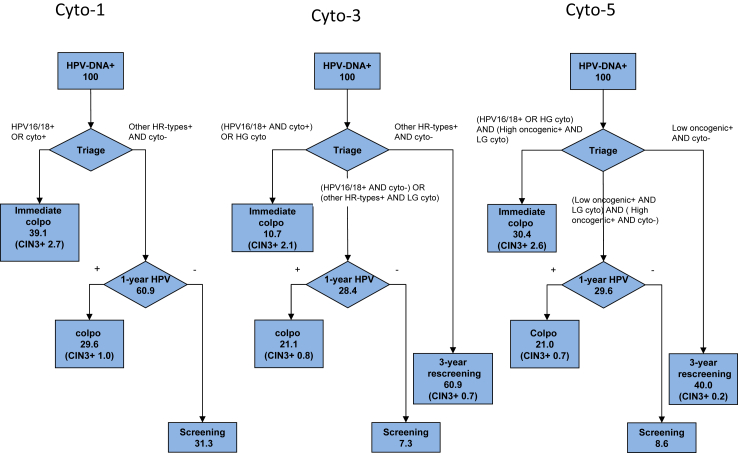
Background: Each high-risk HPV genotype has different oncogenic potential, and the risk of CIN3+ varies according to genotype. We evaluated the performance of different strategies of HPV-positivity triage combining cytology, p16/ki67 dual staining (DS), and extended genotyping.
Methods: Samples from 3180 consecutive women from the NTCC2 study (NCT01837693) positive for HPV DNA at primary screening, were retrospectively analyzed by the BD Onclarity HPV Assay, which allows extended genotyping. Genotypes were divided into three groups based on the risk of CIN3+. HPV DNA-positive women were followed up for 24 months or to clearance.
Findings: Combining the three groups of genotypes with cytology or DS results we identify a group of women who need immediate colposcopy (PPV for CIN3+ from 7.8 to 20.1%), a group that can be referred to 1-year HPV retesting (PPV in those HPV-positive at retesting from 2.2 to 3.8), and a group with a very low 24-month CIN3+ risk, i.e. 0.4%, composed by women cytology or DS negative and positive for HPV 56/59/66 or 35/39/68 or negative with the Onclarity test, who can be referred to 3-year retesting.
Interpretation: Among the baseline HPV DNA positive/cytology or DS negative women, the extended genotyping allows to stratify for risk of CIN3+, and to identify a group of women with a risk of CIN3+ so low in the next 24 months that they could be referred to a new screening round after 3 years.
Funding: Italian Ministry of Health (grant number RF-2009-1536040). Hologic-Genprobe, Roche Diagnostics, and Becton & Dickinson provided financial and non-financial support.
Keywords: Accuracy; Cervical cancer screening; Cervical intraepithelial neoplasia; HPV DNA testing; HPV genotyping; Human papillomavirus; Triage; p16/ki67 dual staining.
Copyright © 2024 The Authors. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Declaration of interests Maria Benevolo and Paolo Giorgi Rossi as principal investigator and former PI of the NTCC2 study reports nonfinancial support from Roche Diagnostics and Hologic S. r.l., which provided part of the reagents for free or at reduced price. Moreover, Maria Benevolo, Paolo Giorgi Rossi, Simonetta Bisanzi, and Laura De Marco obtained financial and nonfinancial support from Becton & Dickinson. Maria Benevolo also reports financial and nonfinancial support from Arrow S. r.l. for works outside this project. All other authors declare no conflict of interests.
Figures



References
-
- Ronco G., Arbyn M., Meijer C.J., Snijeders P., Cuzick J. In: European guidelines for quality assurance in cervical cancer screening. Second, Supplement ed. Anttila A., Arbyn M., De Vuyst H., et al., editors. Office for Official Publications of the European Union; Luxembourg: 2015. Screening for cervical cancer with primary testing for human papillomavirus; pp. 1–68.
-
- WHO guideline for screening and treatment of cervical pre-cancer lesions for cervical cancer prevention. 2nd ed. 2021. Geneva. - PubMed
-
- Anttila A., Arbyn M., De Vuyst H., et al. Publications Office; Luxembourg: 2015. European guidelines for quality assurance in cervical cancer screening.http://dx.publications.europa.eu/10.2875/93363 - DOI
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
