

Impact of Anatomical and Viability-Guided Completeness of Revascularization on Clinical Outcomes in Ischemic Cardiomyopathy
- PMID: 38759904
- PMCID: PMC11250908
- DOI: 10.1016/j.jacc.2024.04.043
Impact of Anatomical and Viability-Guided Completeness of Revascularization on Clinical Outcomes in Ischemic Cardiomyopathy
Abstract
Background: Complete revascularization of coronary artery disease has been linked to improved outcomes in patients with preserved left ventricular (LV) function.
Objectives: This study sought to identify the impact of complete revascularization in patients with severe LV dysfunction.
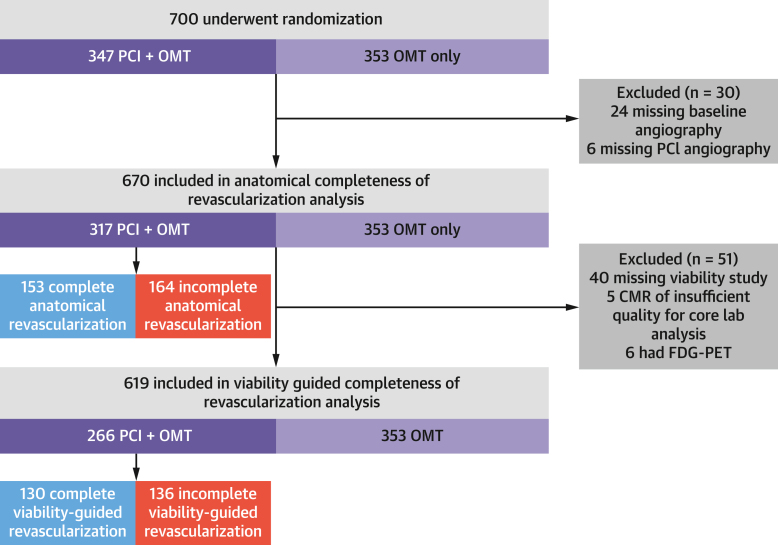
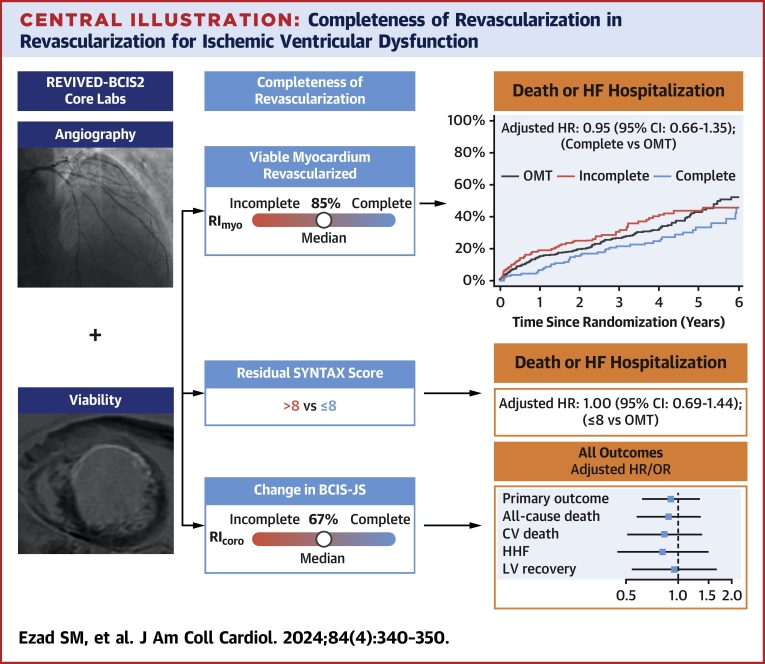
Methods: Patients enrolled in the REVIVED-BCIS2 (Revascularization for Ischemic Ventricular Dysfunction) trial were eligible if baseline/procedural angiograms and viability studies were available for analysis by independent core laboratories. Anatomical and viability-guided completeness of revascularization were measured by the coronary and myocardial revascularization indices (RIcoro and RImyo), respectively, where RIcoro = (change in British Cardiovascular Intervention Society Jeopardy score [BCIS-JS]) / (baseline BCIS-JS) and RImyo= (number of revascularized viable segments) / (number of viable segments supplied by diseased vessels). The percutaneous coronary intervention (PCI) group was classified as having complete or incomplete revascularization by median RIcoro and RImyo. The primary outcome was death or hospitalization for heart failure.
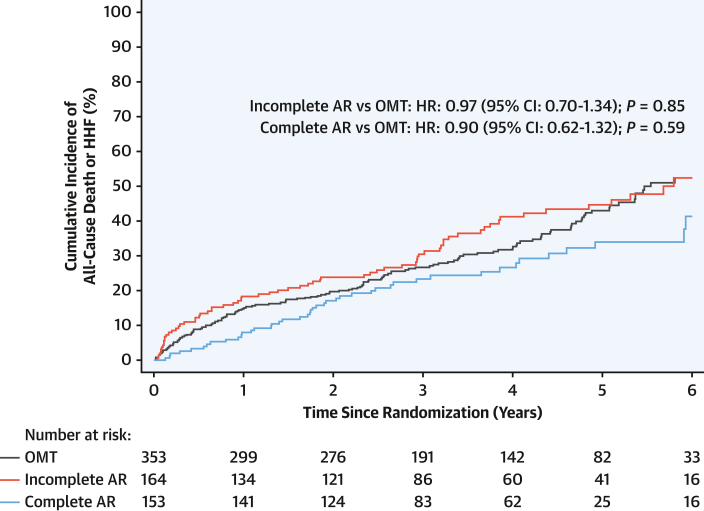
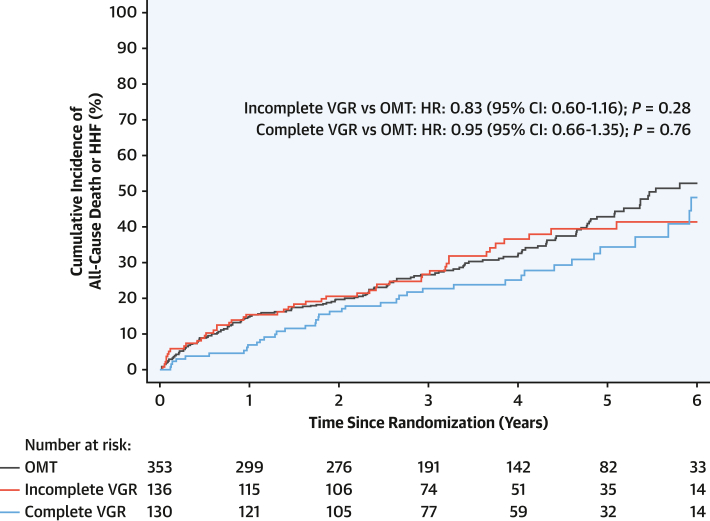
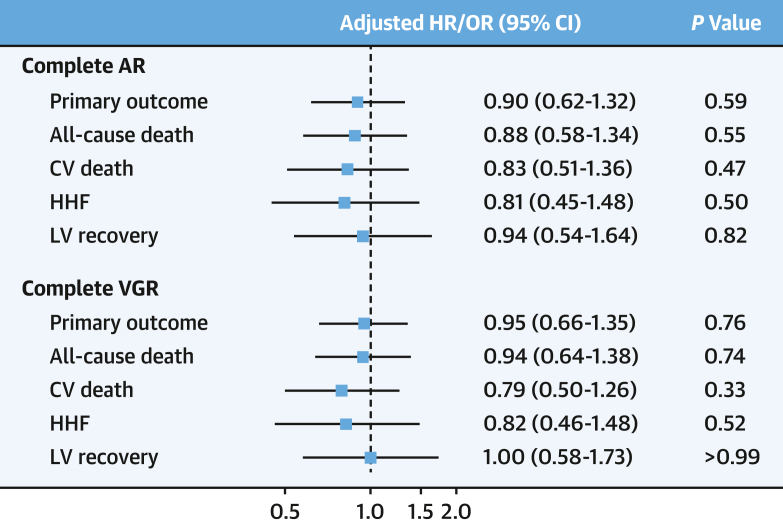
Results: Of 700 randomized patients, 670 were included. The baseline BCIS-JS and SYNTAX (Synergy Between PCI With Taxus and Cardiac Surgery) scores were 8 (Q1-Q3: 6-10) and 22 (Q1-Q3: 15-29), respectively. In those patients assigned to PCI, median RIcoro and RImyo values were 67% and 85%, respectively. Compared with the group assigned to optimal medical therapy alone, there was no difference in the likelihood of the primary outcome in those patients receiving complete anatomical or viability-guided revascularization (HR: 0.90; 95% CI: 0.62-1.32; and HR: 0.95; 95% CI: 0.66-1.35, respectively). A sensitivity analysis by residual SYNTAX score showed no association with outcome.
Conclusions: In patients with severe LV dysfunction, neither complete anatomical nor viability-guided revascularization was associated with improved event-free survival compared with incomplete revascularization or treatment with medical therapy alone. (Revascularization for Ischemic Ventricular Dysfunction) [REVIVED-BCIS2]; NCT01920048).
Keywords: complete revascularization; heart failure; left ventricular dysfunction; percutaneous coronary intervention; stable coronary artery disease.
Copyright © 2024 The Authors. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Funding Support and Author Disclosures The trial was funded by the National Institute for Health and Care Research (UK) Health Technology Assessment Program (NIHR 10/57/67); and the present work was supported by the British Heart Foundation (FS/CRTF/21/24118, RE/18/2/34213 and RE/18/6/34217). The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Figures
References
-
- Neumann F.J., Sousa-Uva M., Ahlsson A., et al. 2018 ESC/EACTS guidelines on myocardial revascularization. Eur Heart J. 2019;40:87–165. - PubMed
-
- Garcia S., Sandoval Y., Roukoz H., et al. Outcomes after complete versus incomplete revascularization of patients with multivessel coronary artery disease: a meta-analysis of 89,883 patients enrolled in randomized clinical trials and observational studies. J Am Coll Cardiol. 2013;62:1421–1431. - PubMed
-
- Perera D., Clayton T., O’Kane P.D., et al. Percutaneous revascularization for ischemic left ventricular dysfunction. N Engl J Med. 2022;387:1351–1360. - PubMed
-
- Perera D., Clayton T., Petrie M.C., et al. Percutaneous revascularization for ischemic ventricular dysfunction: rationale and design of the REVIVED-BCIS2 trial: percutaneous coronary intervention for ischemic cardiomyopathy. JACC Heart Fail. 2018;6:517–526. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
