

Future perspective and clinical applicability of the combined use of plasma phosphorylated tau 181 and neurofilament light chain in Subjective Cognitive Decline and Mild Cognitive Impairment
- PMID: 38760423
- PMCID: PMC11101654
- DOI: 10.1038/s41598-024-61655-6
Future perspective and clinical applicability of the combined use of plasma phosphorylated tau 181 and neurofilament light chain in Subjective Cognitive Decline and Mild Cognitive Impairment
Abstract
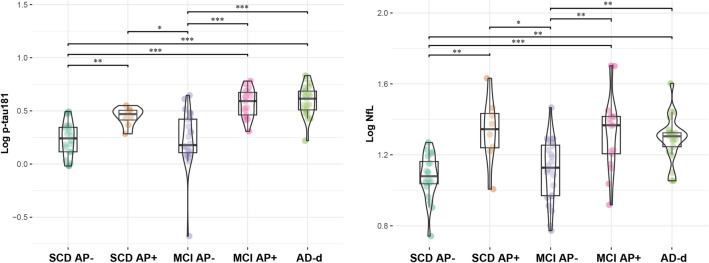
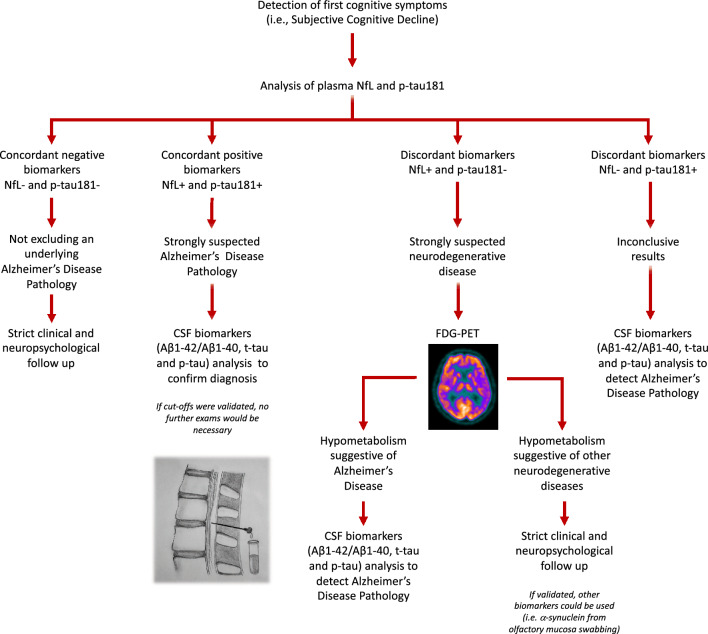
We aimed to assess diagnostic accuracy of plasma p-tau181 and NfL separately and in combination in discriminating Subjective Cognitive Decline (SCD) and Mild Cognitive Impairment (MCI) patients carrying Alzheimer's Disease (AD) pathology from non-carriers; to propose a flowchart for the interpretation of the results of plasma p-tau181 and NfL. We included 43 SCD, 41 MCI and 21 AD-demented (AD-d) patients, who underwent plasma p-tau181 and NfL analysis. Twenty-eight SCD, 41 MCI and 21 AD-d patients underwent CSF biomarkers analysis (Aβ1-42, Aβ1-42/1-40, p-tau, t-tau) and were classified as carriers of AD pathology (AP+) it they were A+/T+ , or non-carriers (AP-) when they were A-, A+/T-/N-, or A+/T-/N+ according to the A/T(N) system. Plasma p-tau181 and NfL separately showed a good accuracy (AUC = 0.88), while the combined model (NfL + p-tau181) showed an excellent accuracy (AUC = 0.92) in discriminating AP+ from AP- patients. Plasma p-tau181 and NfL results were moderately concordant (Coehn's k = 0.50, p < 0.001). Based on a logistic regression model, we estimated the risk of AD pathology considering the two biomarkers: 10.91% if both p-tau181 and NfL were negative; 41.10 and 76.49% if only one biomarker was positive (respectively p-tau18 and NfL); 94.88% if both p-tau181 and NfL were positive. Considering the moderate concordance and the risk of presenting an underlying AD pathology according to the positivity of plasma p-tau181 and NfL, we proposed a flow chart to guide the combined use of plasma p-tau181 and NfL and the interpretation of biomarker results to detect AD pathology.
Keywords: Alzheimer’s Disease; Mild Cognitive Impairment; NfL; Plasma biomarkers; Subjective Cognitive Decline; p-tau181.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Sperling RA, Aisen PS, Beckett LA, et al. Toward defining the preclinical stages of Alzheimer’s disease: Recommendations from the national institute on aging-Alzheimer’s association workgroups on diagnostic guidelines for Alzheimer’s disease. Alz. Dement. 2011;7(3):280–292. doi: 10.1016/j.jalz.2011.03.003. - DOI - PMC - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
