

Platelet-rich plasma (PRP) treatment of the ovaries significantly improves fertility parameters and reproductive outcomes in diminished ovarian reserve patients: a systematic review and meta-analysis
- PMID: 38760869
- PMCID: PMC11100055
- DOI: 10.1186/s13048-024-01423-2
Platelet-rich plasma (PRP) treatment of the ovaries significantly improves fertility parameters and reproductive outcomes in diminished ovarian reserve patients: a systematic review and meta-analysis
Abstract
Introduction: The incidence of infertility caused by diminished ovarian reserve has become a significant problem worldwide. The beneficial effect of PRP treatment of the ovaries has already been described, but the high-level evidence of its effectiveness has not yet been proven.
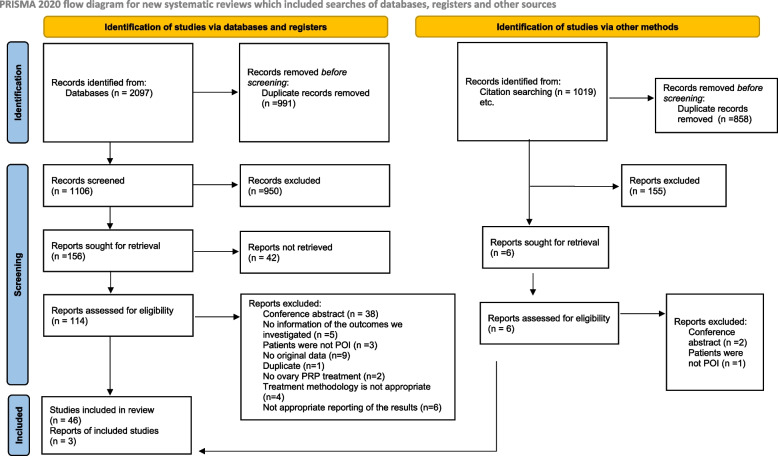
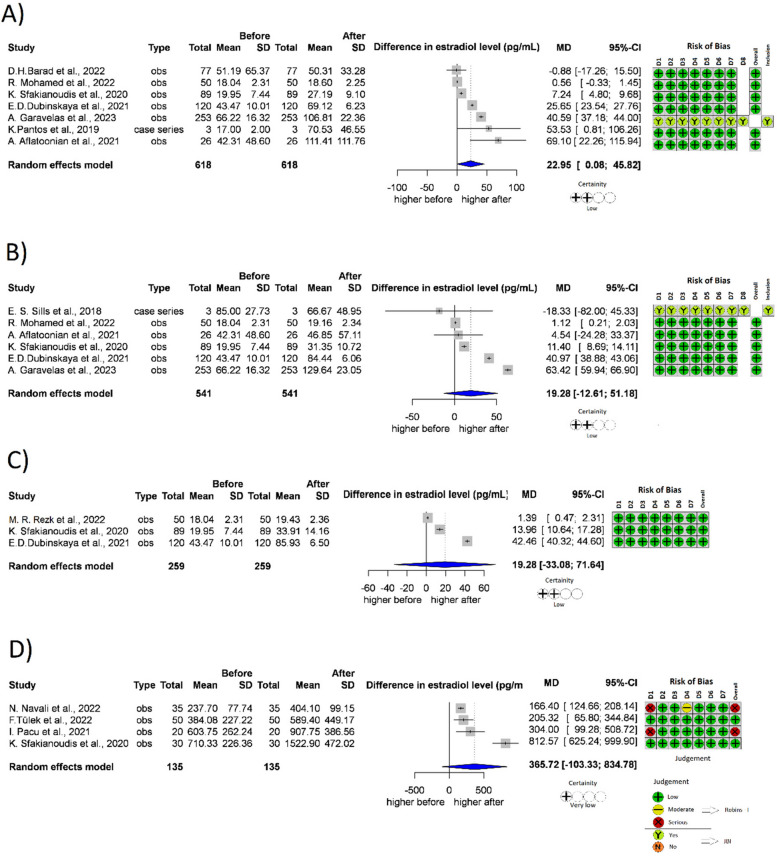
Materials and methods: A systematic search was performed in five databases, until March 12th, 2024. Both randomized and non-randomized studies that compared PRP treatment of the ovaries to self-control among women with diminished ovarian reserve were eligible for inclusion. Hormonal levels (Anti-Müllerian hormone (AMH), Follicle stimulating hormone (FSH), Luteinizing hormone (LH), Estradiol (E2), In-vitro fertilization parameters (Antral follicle count, oocyte, and embryo count), biochemical and spontaneous pregnancy and livebirth were measured.
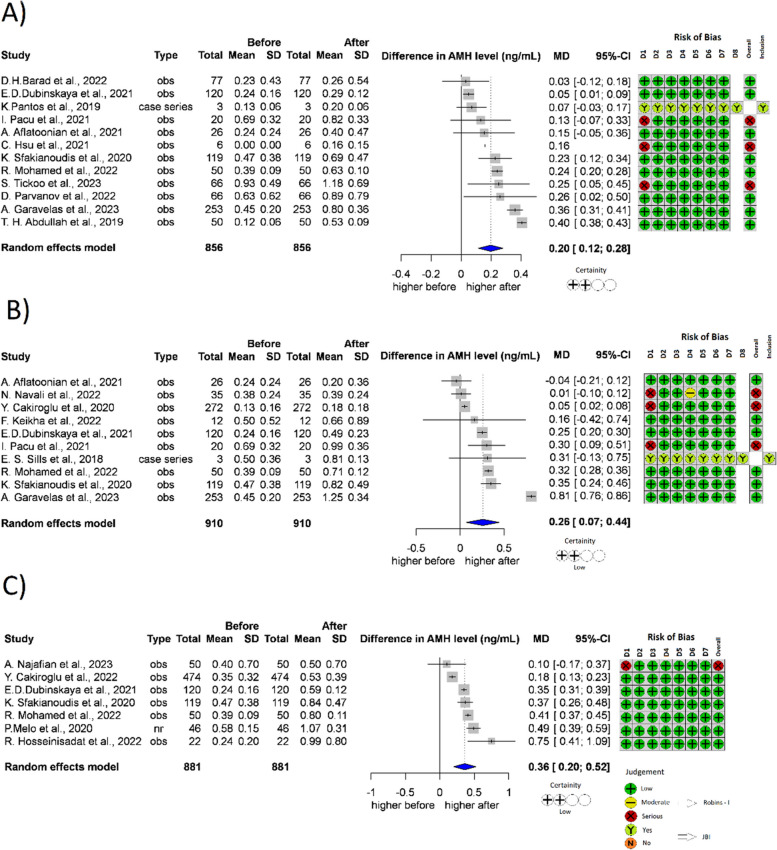
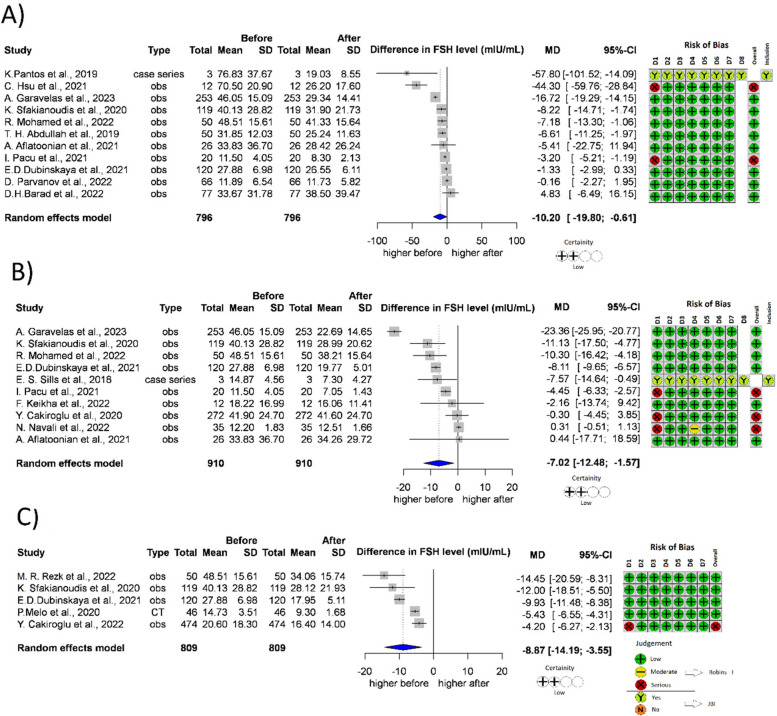
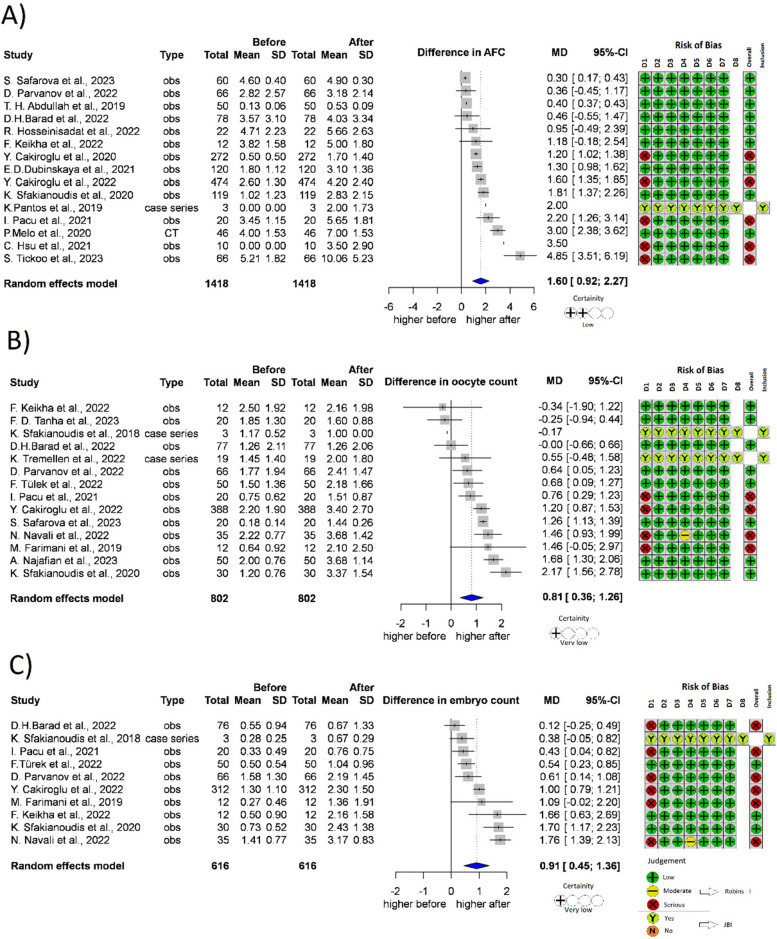
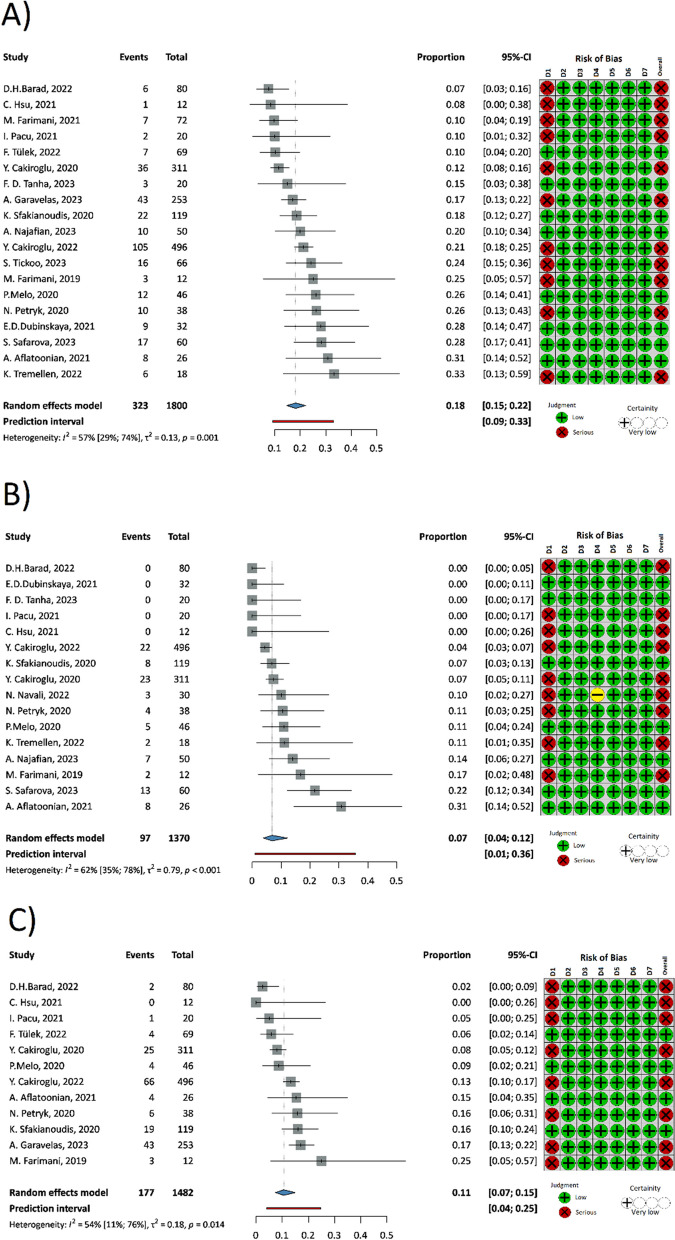
Results: 38 eligible studies were identified reporting on 2256 women. The level of AMH rised, the level of FSH decreased significantly after the PRP treatment. AMH 1 month MD 0.20 (n = 856, p > 0.001, 95% CI: [0.12;0.28]), 2 months MD 0.26 (n = 910, p = 0.013, 95% CI: [0.07;0.44]), 3 months MD 0.36 (n = 881, p = 0.002,95% CI: [0.20;0.52]). FSH 1 month MD -10.20 (n = 796, p > 0.039, 95% CI: [-19.80;-0.61]), 2 months MD -7.02 (n = 910, p = 0.017, 95% CI: [-12.48; -1.57]), 3 months MD -8.87 (n = 809, p = 0.010, 95% CI: [-14.19; -3.55]). The antral follicle count elevated significantly MD 1.60 (n = 1418, p = < 0.001, 95% CI: [0.92; 2.27]). Significant improvement was observed in the number of retrieved oocytes MD 0.81 (n = 802, p = 0.002, 95% CI: [0.36; 1.26]), and embryos created MD 0.91 (n = 616, p = 0.001, 95% CI: [0.45;1.36]). The incidence of spontaneous pregnancy following PRP treatment showed a rate with a proportion of 0.07 (n = 1370, 95% CI: 0.04-0.12), the rate of biochemical pregnancy was 0.18 (n = 1800, 95% CI: 0.15-0.22), livebirth was 0.11 (n = 1482, 95% CI: 0.07-0.15).
Conclusions: Our meta-analysis showed that based on protocolized analysis of the widest scientific literature search to date, containing predominantly observational studies, PRP treatment resulted in a statistically significant improvement in the main fertility parameters of diminished ovarian reserve women. Further multicenter, randomized trials, with large patient numbers and a longer follow-up period are needed to certify our results and develop the most effective treatment protocol.
Keywords: DOR; Diminished ovarian reserve; POF; PRP; Platelet-rich plasma; Premature ovarian failure.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
The authors declare no competing interests.
Figures
References
-
- WHO. Infertility prevalence estimates, 1990–2021. Geneva: World Health Organization; 2023. Licence: CC BY-NC-SA 3.0 IGO.
-
- OECD Family database [Available from: www.oecd.org/els/family/database.htm Accessed 10 October 2023.
-
- The EshreGuidelineGrouponPOI. Webber L, Davies M, Anderson R, Bartlett J, Braat D, et al. ESHRE Guideline: management of women with premature ovarian insufficiency†. Human Reproduction. 2016;31(5):926–37. - PubMed
-
- Pellicer A, Ardiles G, Neuspiller F, Remohí J, Simón C, Bonilla-Musoles F. Evaluation of the ovarian reserve in young low responders with normal basal levels of follicle-stimulating hormone using three-dimensional ultrasonography. Fertil Steril. 1998;70(4):671–675. - PubMed
-
- Herraiz S, Romeu M, Buigues A, Martínez S, Díaz-García C, Gómez-Seguí I, et al. Autologous stem cell ovarian transplantation to increase reproductive potential in patients who are poor responders. Fertil Steril. 2018;110(3):496–505.e1. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
