

Acetabular fractures in geriatric patients: epidemiology, pathomechanism, classification and treatment options
- PMID: 38761237
- PMCID: PMC11576779
- DOI: 10.1007/s00402-024-05312-7
Acetabular fractures in geriatric patients: epidemiology, pathomechanism, classification and treatment options
Abstract
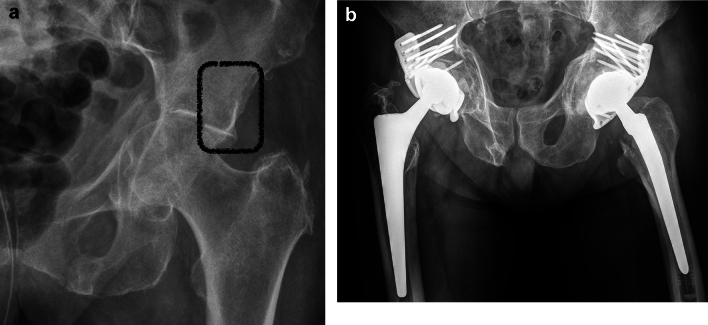
The incidence of geriatric acetabular fractures has shown a sharp increase in the last decades. The majority of patients are male, which is different to other osteoporotic fractures. The typical pathomechanism generally differs from acetabular fractures in young patients regarding both the direction and the amount of force transmission to the acetabulum via the femoral head. Geriatric fractures very frequently involve anterior structures of the acetabulum, while the posterior wall is less frequently involved. The anterior column and posterior hemitransverse (ACPHT) fracture is the most common fracture type. Superomedial dome impactions (gull sign) are a frequent feature in geriatric acetabular fractures as well. Treatment options include nonoperative treatment, internal fixation and arthoplasty. Nonoperative treatment includes rapid mobilisation and full weighbearing under analgesia and is advisable in non- or minimally displaced fractures without subluxation of the hip joint and without positive gull sign. Open reduction and internal fixation of geriatric acetabular fractures leads to good or excellent results, if anatomic reduction is achieved intraoperatively and loss of reduction does not occur postoperatively. Primary arthroplasty of geriatric acetabular fractures is a treatment option, which does not require anatomic reduction, allows for immediate postoperative full weightbearing and obviates several complications, which are associated with internal fixation. The major issue is the fixation of the acetabular cup in the fractured bone. Primary cups, reinforcement rings or a combination of arthroplasty and internal fixation may be applied depending on the acetabular fracture type.
Keywords: Anterior column and posterior hemitransverse fracture; Geriatric acetabular fracture; Gull sign; Internal fixation; Primary arthroplasty.
© 2024. The Author(s).
Conflict of interest statement
Figures


References
-
- Hoellen IP, Mentzel M, Bischoff M, Kinzl L (1997) Acetabular fractures in the elderly––primary endopprosthetis. Orthopade 26(4):348–353. 10.1007/PL00003390 - PubMed
-
- Ochs BG, Marintschev I, Hoyer H, Rolauffs B, Culemann U, Pohlemann T, Stuby FM (2010) Changes in the treatment of acetabular fractures over 15 years: analysis of 1266 cases treated by the German pelvic multicentre study group (DAO/DGU). Injury 41(8):839–851. 10.1016/j.injury.2010.04.010 - PubMed
-
- Toro JB, Hierholzer C, Helfet DL (2004) Acetabular fractures in the elderly. Bull Hosp Jt Dis 62(1–2):53–57 - PubMed
-
- Vanderschot P (2007) Treatment options of pelvic and acetabular fractures in patients with osteoporotic bone. Injury 38(4):497–508. 10.1016/j.injury.2007.01.021 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
