

Bone metabolism in diabetes: a clinician's guide to understanding the bone-glucose interplay
- PMID: 38761257
- PMCID: PMC11343884
- DOI: 10.1007/s00125-024-06172-x
Bone metabolism in diabetes: a clinician's guide to understanding the bone-glucose interplay
Abstract
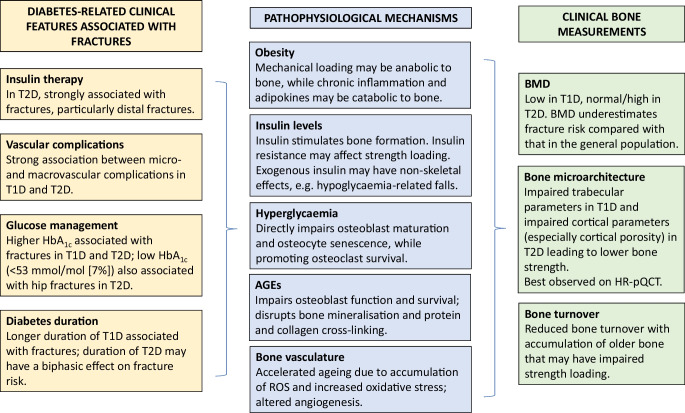
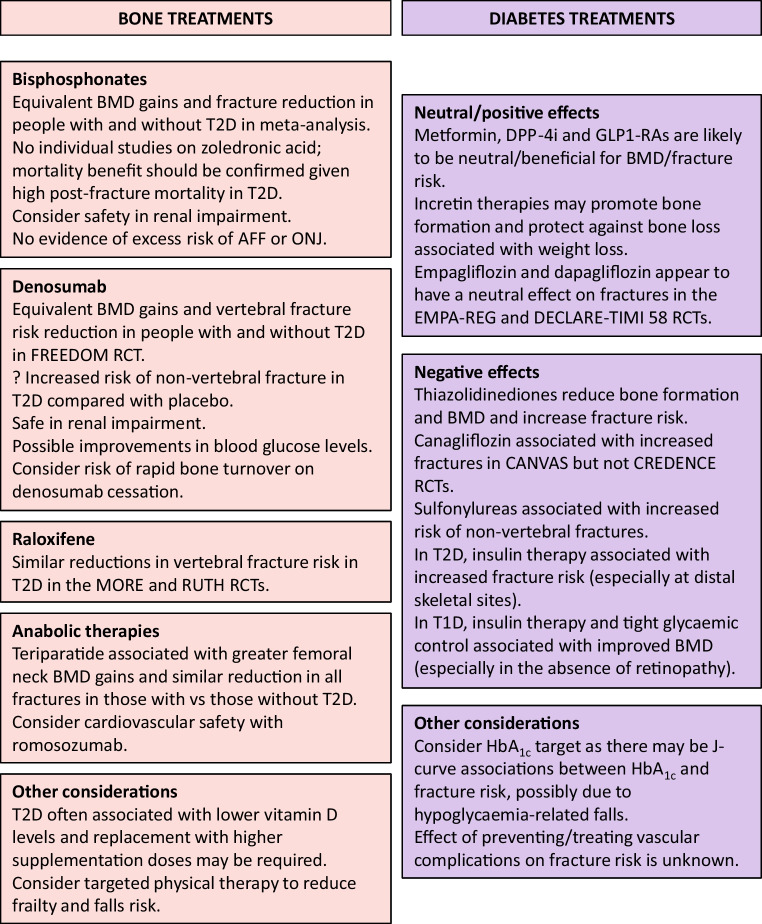
Skeletal fragility is an increasingly recognised, but poorly understood, complication of both type 1 and type 2 diabetes. Fracture risk varies according to skeletal site and diabetes-related characteristics. Post-fracture outcomes, including mortality risk, are worse in those with diabetes, placing these people at significant risk. Each fracture therefore represents a sentinel event that warrants targeted management. However, diabetes is a very heterogeneous condition with complex interactions between multiple co-existing, and highly correlated, factors that preclude a clear assessment of the independent clinical markers and pathophysiological drivers for diabetic osteopathy. Additionally, fracture risk calculators and routinely used clinical bone measurements generally underestimate fracture risk in people with diabetes. In the absence of dedicated prospective studies including detailed bone and metabolic characteristics, optimal management centres around selecting treatments that minimise skeletal and metabolic harm. This review summarises the clinical landscape of diabetic osteopathy and outlines the interplay between metabolic and skeletal health. The underlying pathophysiology of skeletal fragility in diabetes and a rationale for considering a diabetes-based paradigm in assessing and managing diabetic bone disease will be discussed.
Keywords: Bone; Diabetes; Fractures; Insulin resistance; Osteoporosis; Review.
© 2024. The Author(s).
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
