

Application of genetic testing for the diagnosis of von Willebrand disease
- PMID: 38762018
- PMCID: PMC11548015
- DOI: 10.1016/j.jtha.2024.05.006
Application of genetic testing for the diagnosis of von Willebrand disease
Abstract
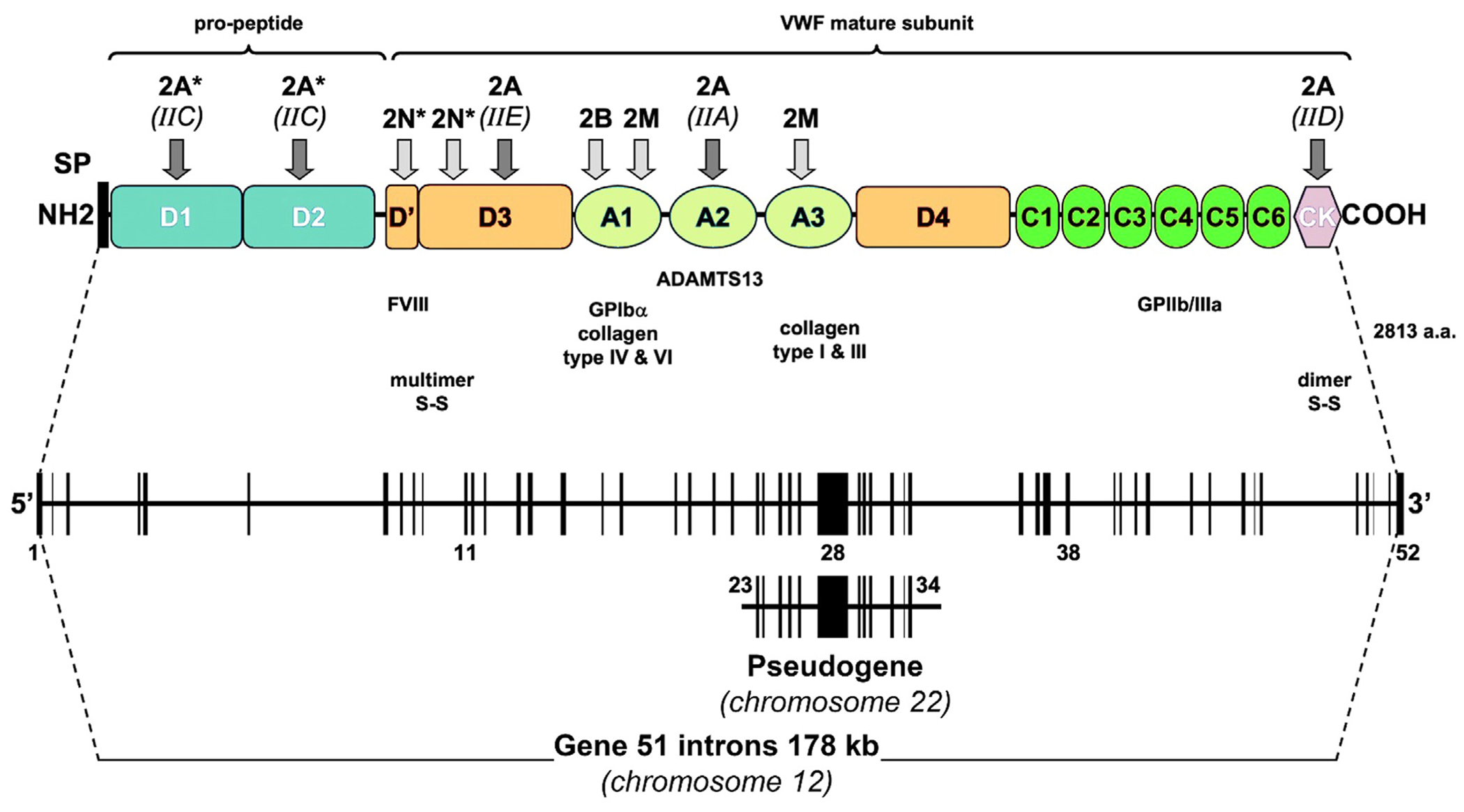
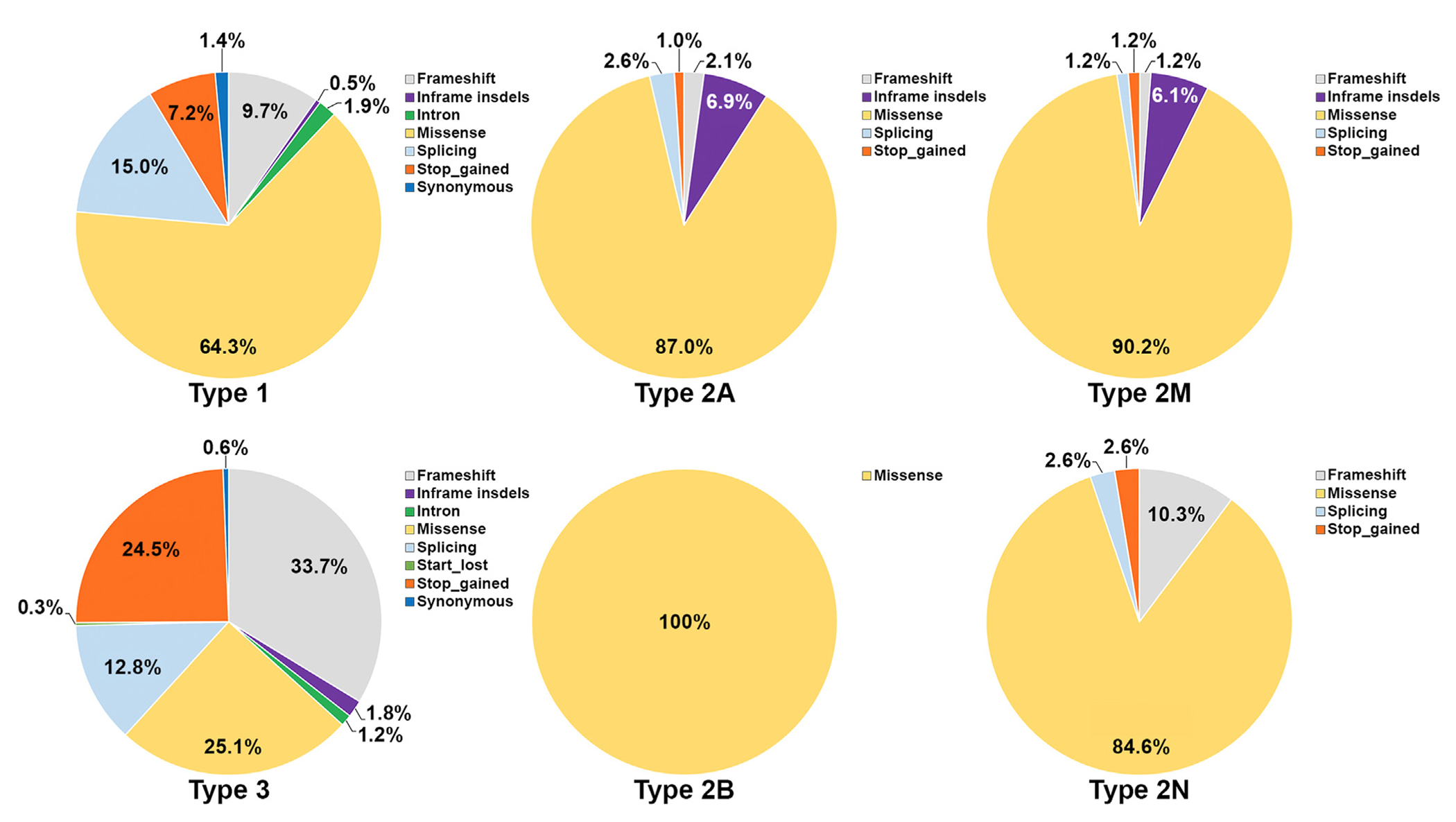
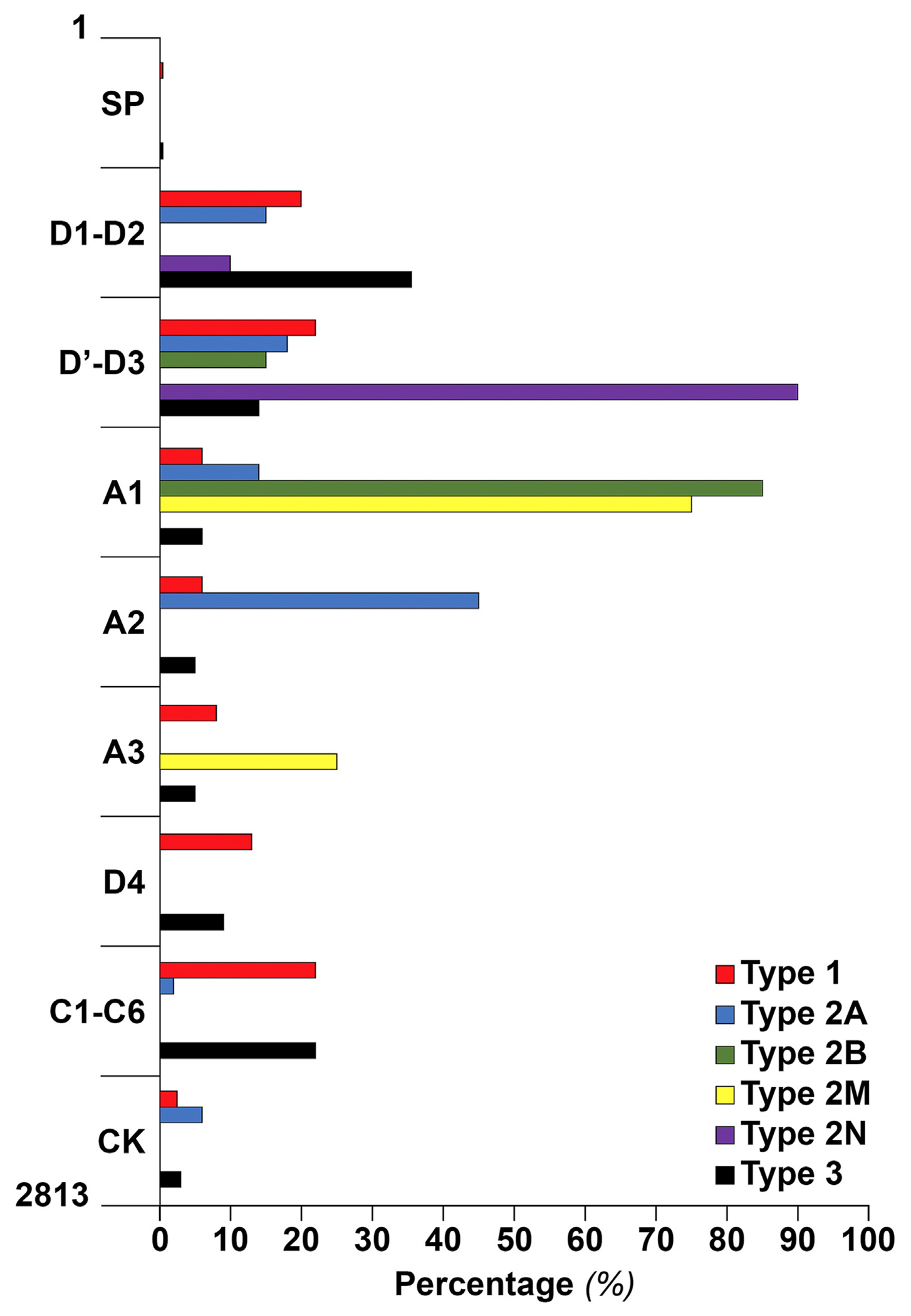
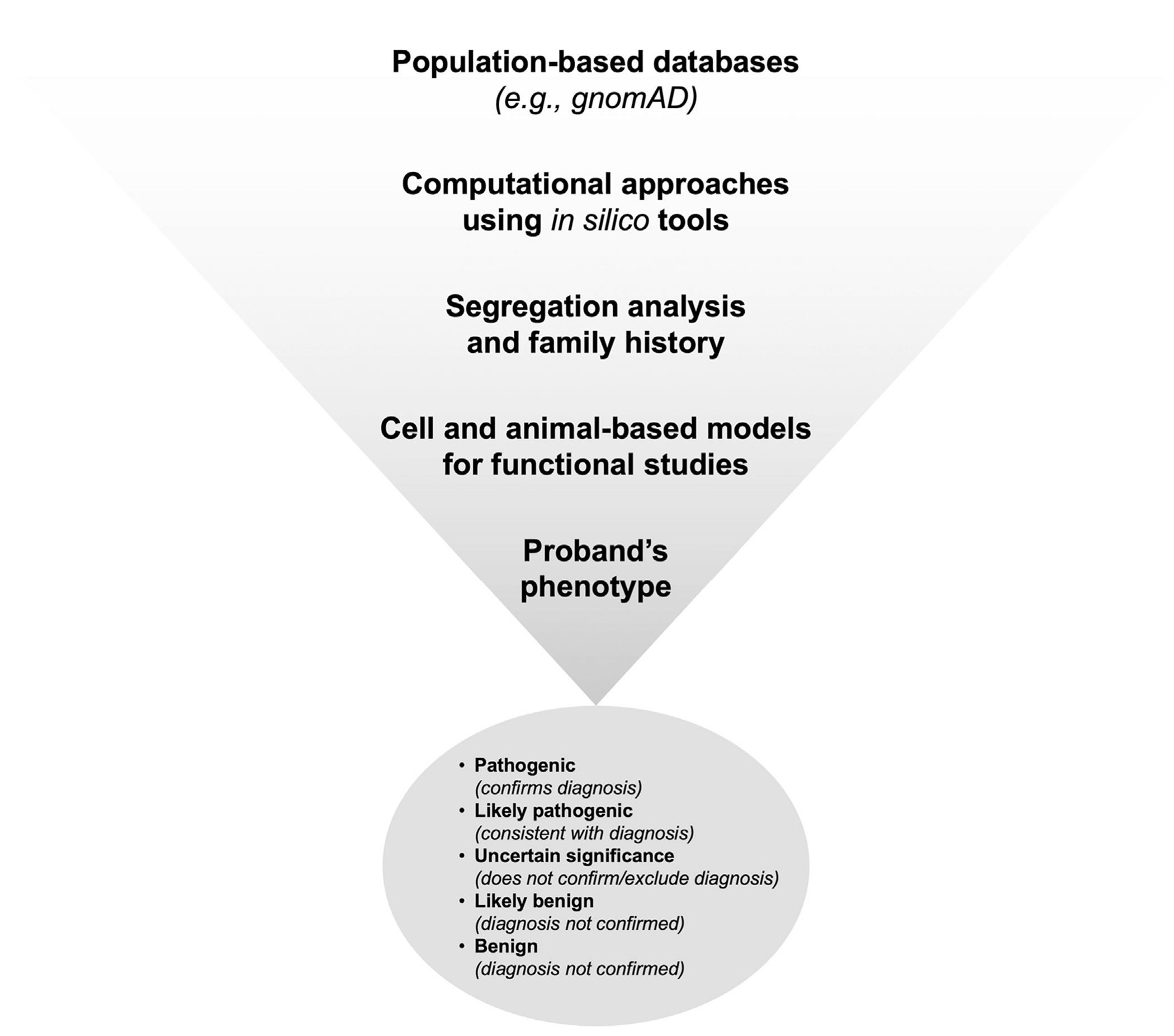
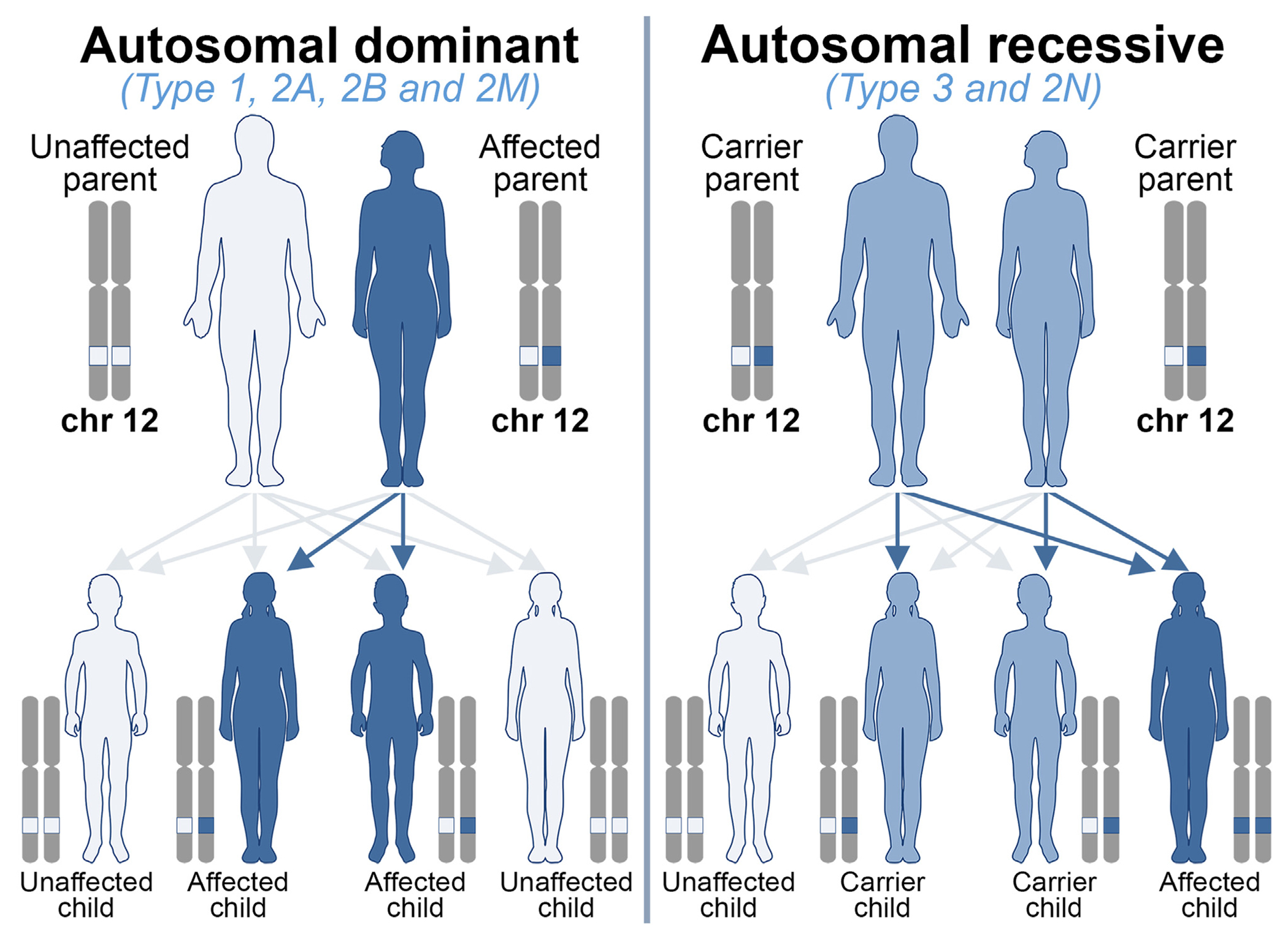
von Willebrand disease (VWD) is the most frequent inherited bleeding disorder, with an estimated symptomatic prevalence of 1 per 1000 in the general population. VWD is characterized by defects in the quantity, quality, or multimeric structure of von Willebrand factor (VWF), a glycoprotein being hemostatically essential in circulation. VWD is classified into 3 principal types: low VWF/type 1 with partial quantitative deficiency of VWF, type 3 with virtual absence of VWF, and type 2 with functional abnormalities of VWF, being classified as 2A, 2B, 2M, and 2N. A new VWD type has been officially recognized by the ISTH SSC on von Willebrand factor which has also been discussed by the joint ASH/ISTH/NHF/WFH 2021 guidelines (ie, type 1C), indicating patients with quantitative deficiency due to an enhanced VWF clearance. With the advent of next-generation sequencing technologies, the process of genetic diagnosis has substantially changed and improved accuracy. Therefore, nowadays, patients with type 3 and severe type 1 VWD can benefit from genetic testing as much as type 2 VWD. Specifically, genetic testing can be used to confirm or differentiate a VWD diagnosis, as well as to provide genetic counseling. The focus of this manuscript is to discuss the current knowledge on VWD molecular pathophysiology and the application of genetic testing for VWD diagnosis.
Keywords: NGS; VWD; VWF; genetic testing; molecular diagnosis.
Copyright © 2024 International Society on Thrombosis and Haemostasis. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of competing interests F.P. serves on the advisory committee of CSL-Behring, BioMarin, Roche, Sanofi, and Sobi and participated in educational meetings/symposia of Takeda/Spark. D.L. reports research support from BioMarin, CSL-Behring, and Sanofi and participates in an advisory role for BioMarin, CSL-Behring, Novo Nordisk, and Pfizer. The other authors state that they have no conflict of interest.
Figures
Similar articles
-
Clinical, Phenotypic and Genotypic Characteristics of Von Willebrand Disease in Afro-Caribbeans: Results From a Study in Martinique Island, French West Indies.Haemophilia. 2025 May;31(3):458-476. doi: 10.1111/hae.70003. Epub 2025 Mar 23. Haemophilia. 2025. PMID: 40123275 Free PMC article.
-
Genetic study of von Willebrand factor antigen levels ≤ 50 IU/dL identifies variants associated with increased risk of von Willebrand disease and bleeding.J Thromb Haemost. 2025 Aug;23(8):2410-2421. doi: 10.1016/j.jtha.2025.04.029. Epub 2025 May 12. J Thromb Haemost. 2025. PMID: 40368142
-
Ratio of Von Willebrand Collagen Binding Assay and Von Willebrand Antigen Can Predict Multimer Size in Von Willebrand Disease.Haemophilia. 2025 May;31(3):450-457. doi: 10.1111/hae.70025. Epub 2025 Mar 7. Haemophilia. 2025. PMID: 40052420 Free PMC article.
-
2025 ASH ISTH NBDF WFH monitoring report on the 2021 clinical guidelines on the diagnosis and management of von Willebrand disease.Blood Adv. 2025 Jul 22;9(14):3553-3555. doi: 10.1182/bloodadvances.2025016512. Blood Adv. 2025. PMID: 40273329 Free PMC article. Review.
-
Von Willebrand factor is a multifaceted player in hemostasis requiring a diverse array of analytical and diagnostic approaches.Expert Rev Hematol. 2025 Jul 9:1-18. doi: 10.1080/17474086.2025.2525458. Online ahead of print. Expert Rev Hematol. 2025. PMID: 40555973 Review.
Cited by
-
Global prevalence of platelet-type von Willebrand disease.Res Pract Thromb Haemost. 2025 Jan 16;9(1):102682. doi: 10.1016/j.rpth.2025.102682. eCollection 2025 Jan. Res Pract Thromb Haemost. 2025. PMID: 39975577 Free PMC article.
-
Challenges and considerations of genetic testing in von Willebrand disease.Res Pract Thromb Haemost. 2025 Jan 16;9(1):102686. doi: 10.1016/j.rpth.2025.102686. eCollection 2025 Jan. Res Pract Thromb Haemost. 2025. PMID: 39975579 Free PMC article. Review.
-
Comparison of genotypes and phenotypes for von Willebrand factor gene variants using Japanese genome database.Blood Vessel Thromb Hemost. 2025 Apr 10;2(3):100070. doi: 10.1016/j.bvth.2025.100070. eCollection 2025 Aug. Blood Vessel Thromb Hemost. 2025. PMID: 40765908 Free PMC article.
References
-
- Rodeghiero F, Castaman G, Dini E. Epidemiological investigation of the prevalence of von Willebrand’s disease. Blood. 1987;69:454–9. - PubMed
-
- Werner EJ, Broxson EH, Tucker EL, Giroux DS, Shults J, Abshire TC. Prevalence of von Willebrand disease in children: a multiethnic study. J Pediatr. 1993;123:893–8. - PubMed
-
- Bowman M, Hopman W, Rapson D, Lillicrap D, James P. The prevalence of symptomatic von Willebrand disease in primary care practice. J Thromb Haemost. 2010;8:213–6. - PubMed
-
- Sadler JE, Budde U, Eikenboom JC, Favaloro EJ, Hill FG, Holmberg L, Ingerslev J, Lee CA, Lillicrap D, Mannucci PM, Mazurier C, Meyer D, Nichols WL, Nishino M, Peake IR, Rodeghiero F, Schneppenheim R, Ruggeri ZM, Srivastava A, Montgomery RR, et al. Update on the pathophysiology and classification of von Willebrand disease: a report of the Subcommittee on von Willebrand Factor. J Thromb Haemost. 2006;4:2103–14. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
