

AI-enhanced integration of genetic and medical imaging data for risk assessment of Type 2 diabetes
- PMID: 38762475
- PMCID: PMC11102564
- DOI: 10.1038/s41467-024-48618-1
AI-enhanced integration of genetic and medical imaging data for risk assessment of Type 2 diabetes
Abstract
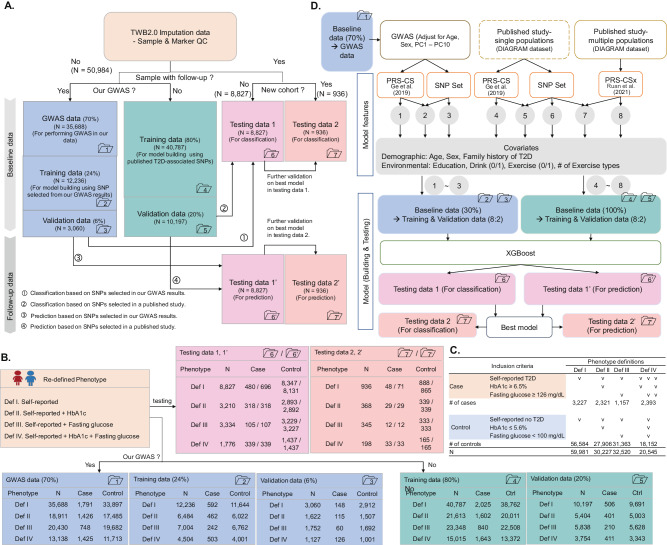
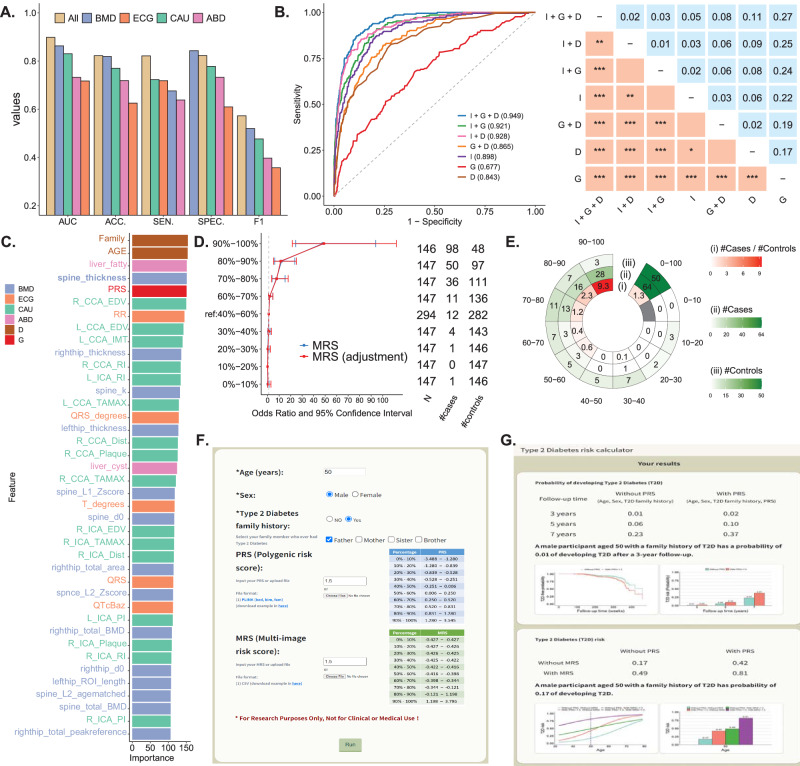
Type 2 diabetes (T2D) presents a formidable global health challenge, highlighted by its escalating prevalence, underscoring the critical need for precision health strategies and early detection initiatives. Leveraging artificial intelligence, particularly eXtreme Gradient Boosting (XGBoost), we devise robust risk assessment models for T2D. Drawing upon comprehensive genetic and medical imaging datasets from 68,911 individuals in the Taiwan Biobank, our models integrate Polygenic Risk Scores (PRS), Multi-image Risk Scores (MRS), and demographic variables, such as age, sex, and T2D family history. Here, we show that our model achieves an Area Under the Receiver Operating Curve (AUC) of 0.94, effectively identifying high-risk T2D subgroups. A streamlined model featuring eight key variables also maintains a high AUC of 0.939. This high accuracy for T2D risk assessment promises to catalyze early detection and preventive strategies. Moreover, we introduce an accessible online risk assessment tool for T2D, facilitating broader applicability and dissemination of our findings.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures




References
-
- Chen H-Y, Kuo S, Su P-F, Wu J-S, Ou H-T. Health care costs associated with macrovascular, microvascular, and metabolic complications of type 2 diabetes across time: estimates from a population-based cohort of more than 0.8 million individuals with up to 15 years of follow-up. Diabetes Care. 2020;43:1732–1740. doi: 10.2337/dc20-0072. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
