

Independent relationship between sleep apnea-specific hypoxic burden and glucolipid metabolism disorder: a cross-sectional study
- PMID: 38762509
- PMCID: PMC11102635
- DOI: 10.1186/s12931-024-02846-7
Independent relationship between sleep apnea-specific hypoxic burden and glucolipid metabolism disorder: a cross-sectional study
Abstract
Objectives: Obstructive sleep apnea (OSA) is associated with abnormal glucose and lipid metabolism. However, whether there is an independent association between Sleep Apnea-Specific Hypoxic Burden (SASHB) and glycolipid metabolism disorders in patients with OSA is unknown.
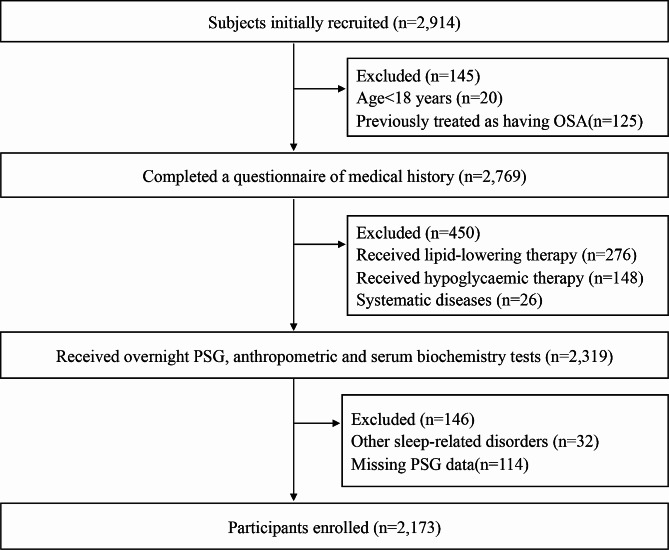
Methods: We enrolled 2,173 participants with suspected OSA from January 2019 to July 2023 in this study. Polysomnographic variables, biochemical indicators, and physical measurements were collected from each participant. Multiple linear regression analyses were used to evaluate independent associations between SASHB, AHI, CT90 and glucose as well as lipid profile. Furthermore, logistic regressions were used to determine the odds ratios (ORs) for abnormal glucose and lipid metabolism across various SASHB, AHI, CT90 quartiles.
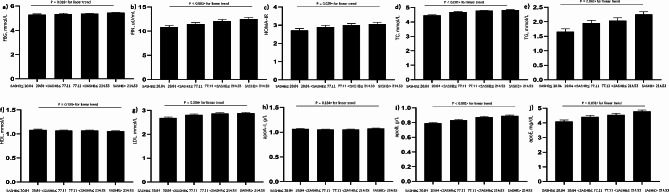
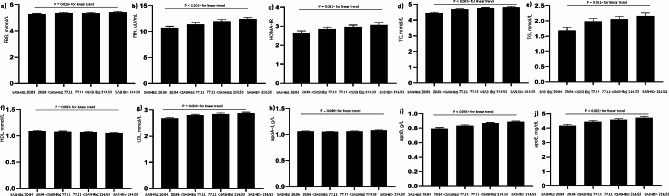
Results: The SASHB was independently associated with fasting blood glucose (FBG) (β = 0.058, P = 0.016), fasting insulin (FIN) (β = 0.073, P < 0.001), homeostasis model assessment of insulin resistance (HOMA-IR) (β = 0.058, P = 0.011), total cholesterol (TC) (β = 0.100, P < 0.001), total triglycerides (TG) (β = 0.063, P = 0.011), low-density lipoprotein cholesterol (LDL-C) (β = 0.075, P = 0.003), apolipoprotein A-I (apoA-I) (β = 0.051, P = 0.049), apolipoprotein B (apoB) (β = 0.136, P < 0.001), apolipoprotein E (apoE) (β = 0.088, P < 0.001) after adjustments for confounding factors. Furthermore, the ORs for hyperinsulinemia across the higher SASHB quartiles were 1.527, 1.545, and 2.024 respectively, compared with the lowest quartile (P < 0.001 for a linear trend); the ORs for hyper-total cholesterolemia across the higher SASHB quartiles were 1.762, 1.998, and 2.708, compared with the lowest quartile (P < 0.001 for a linear trend) and the ORs for hyper-LDL cholesterolemia across the higher SASHB quartiles were 1.663, 1.695, and 2.316, compared with the lowest quartile (P < 0.001 for a linear trend). Notably, the ORs for hyper-triglyceridemia{1.471, 1.773, 2.099} and abnormal HOMA-IR{1.510, 1.492, 1.937} maintained a consistent trend across the SASHB quartiles.
Conclusions: We found SASHB was independently associated with hyperinsulinemia, abnormal HOMA-IR, hyper-total cholesterolemia, hyper-triglyceridemia and hyper-LDL cholesterolemia in Chinese Han population. Further prospective studies are needed to confirm that SASHB can be used as a predictor of abnormal glycolipid metabolism disorders in patients with OSA.
Trial registration: ChiCTR1900025714 { http://www.chictr.org.cn/ }; Prospectively registered on 6 September 2019; China.
Keywords: Abnormal glucose and lipid metabolism.; Obstructive sleep apnea hypopnea syndrome; Sleep apnea-specific hypoxic burden.
© 2024. The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

Similar articles
-
Independent relationships between cardinal features of obstructive sleep apnea and glycometabolism: a cross-sectional study.Metabolism. 2018 Aug;85:340-347. doi: 10.1016/j.metabol.2017.11.021. Epub 2018 Feb 1. Metabolism. 2018. PMID: 29382505
-
Elevated low-density lipoprotein cholesterol is independently associated with obstructive sleep apnea: evidence from a large-scale cross-sectional study.Sleep Breath. 2016 May;20(2):627-34. doi: 10.1007/s11325-015-1262-3. Epub 2015 Sep 30. Sleep Breath. 2016. PMID: 26424733
-
Independent association of vitamin D and insulin resistance in obstructive sleep apnea.Ann Endocrinol (Paris). 2019 Nov;80(5-6):319-323. doi: 10.1016/j.ando.2019.09.004. Epub 2019 Nov 1. Ann Endocrinol (Paris). 2019. PMID: 31759518
-
The use of the sleep apnea-specific hypoxic burden to predict obstructive sleep apnea hypopnea syndrome: Evidence from a large cross-sectional study.Sleep Med. 2023 Nov;111:94-100. doi: 10.1016/j.sleep.2023.09.007. Epub 2023 Sep 7. Sleep Med. 2023. PMID: 37742592
-
Effect of the Interaction between Obstructive Sleep Apnea and Lipoprotein(a) on Insulin Resistance: A Large-Scale Cross-Sectional Study.J Diabetes Res. 2019 Apr 8;2019:9583286. doi: 10.1155/2019/9583286. eCollection 2019. J Diabetes Res. 2019. PMID: 31089476 Free PMC article.
Cited by
-
Association of obstructive sleep apnea with cardiovascular events in acute coronary syndrome patients with dual risk of remnant cholesterol and low-grade inflammation: a post-hoc analysis of the OSA-ACS study.Sleep Breath. 2025 Mar 8;29(1):119. doi: 10.1007/s11325-025-03281-8. Sleep Breath. 2025. PMID: 40056262
-
Independent Association of Sleep Apnea-Specific Hypoxic Burden and Sleep Breathing Impairment Index with Thyroid Function in Obstructive Sleep Apnea: A Retrospective Study.Nat Sci Sleep. 2025 Jul 5;17:1543-1556. doi: 10.2147/NSS.S525750. eCollection 2025. Nat Sci Sleep. 2025. PMID: 40635995 Free PMC article.
-
Sleep Temporal Entropy as a Novel Digital Biomarker of Sleep Fragmentation for Cardiometabolic and Mortality Risk.medRxiv [Preprint]. 2025 Jun 6:2025.06.04.25328946. doi: 10.1101/2025.06.04.25328946. medRxiv. 2025. PMID: 40502576 Free PMC article. Preprint.
References
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
