

Enhanced CD95 and interleukin 18 signalling accompany T cell receptor Vβ21.3+ activation in multi-inflammatory syndrome in children
- PMID: 38762592
- PMCID: PMC11102542
- DOI: 10.1038/s41467-024-48699-y
Enhanced CD95 and interleukin 18 signalling accompany T cell receptor Vβ21.3+ activation in multi-inflammatory syndrome in children
Abstract
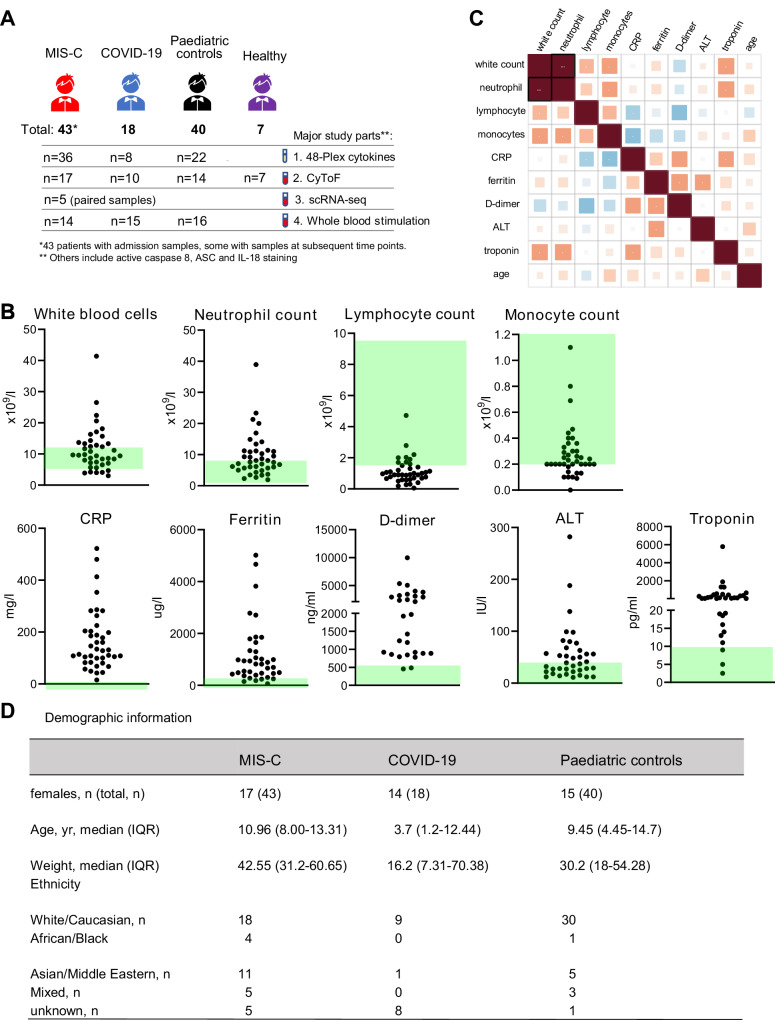
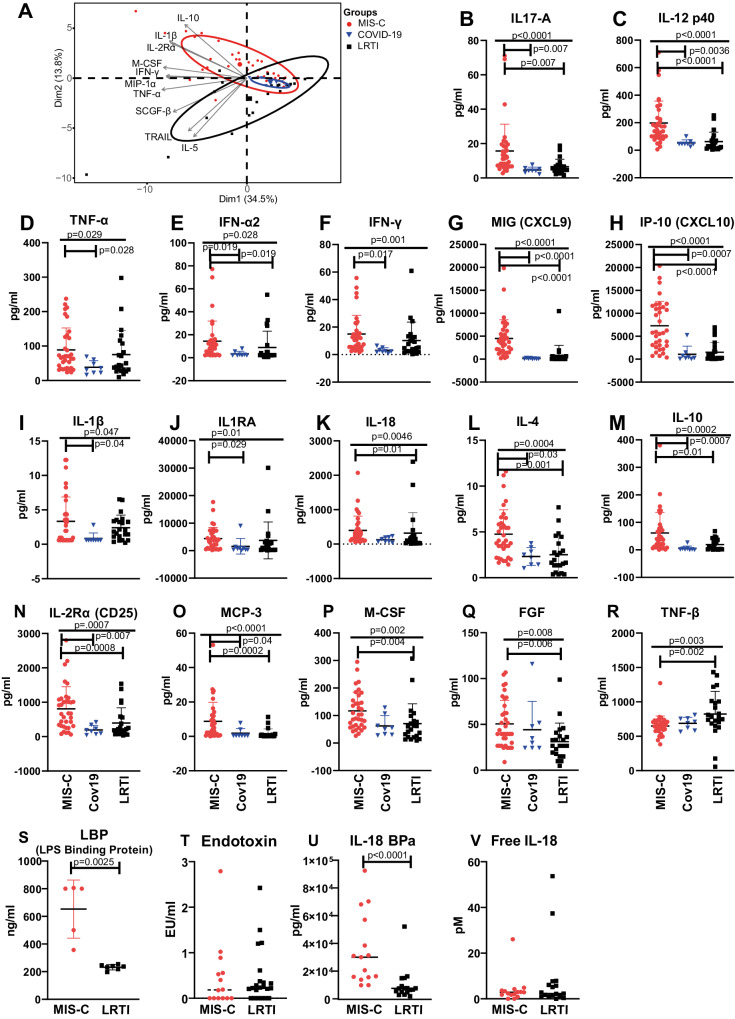
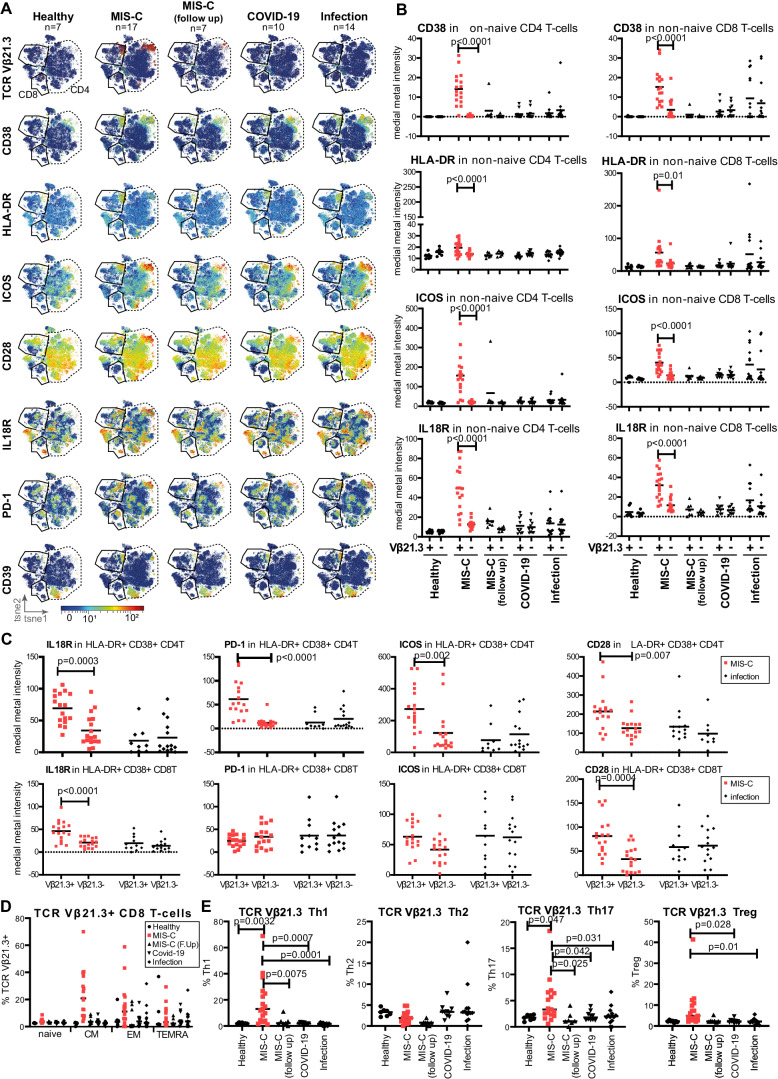
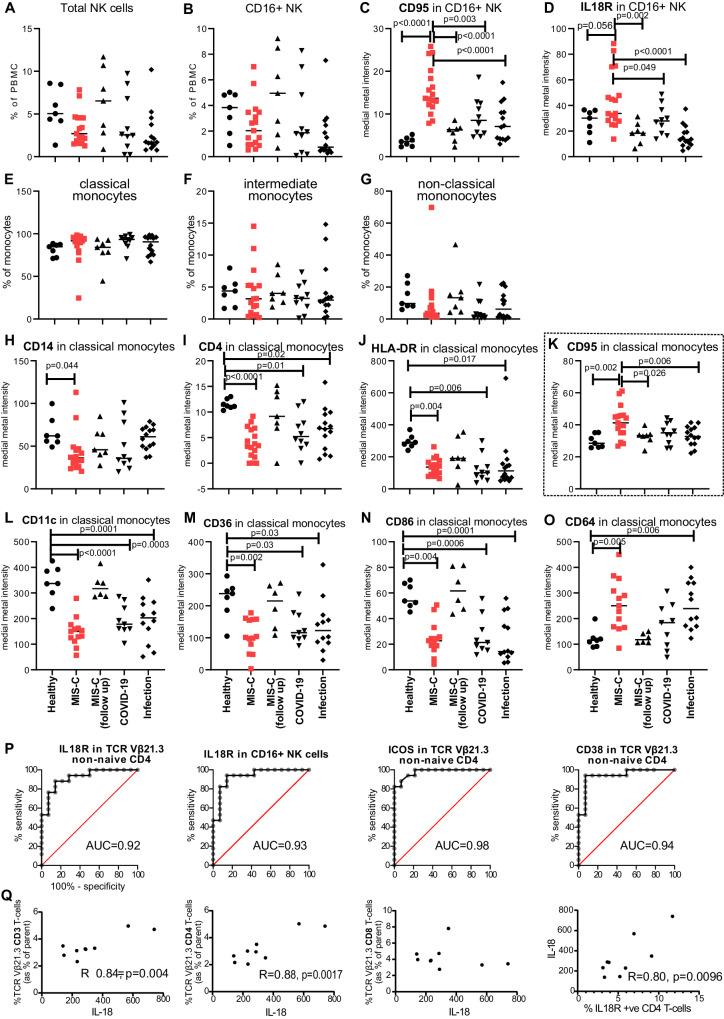
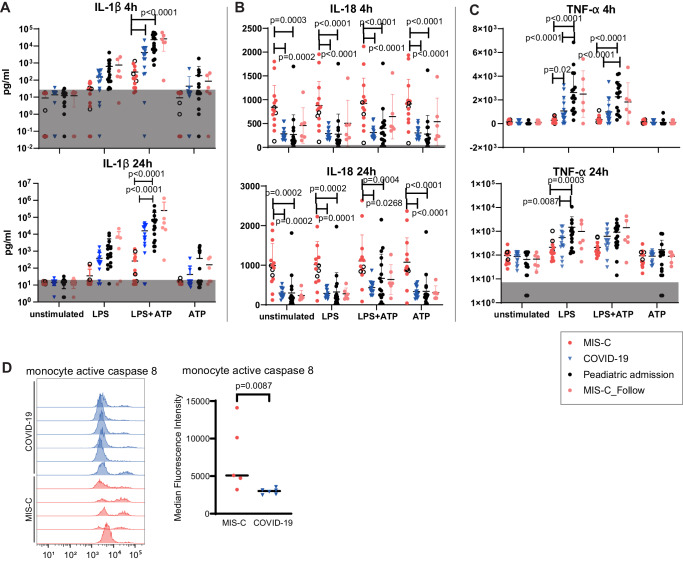
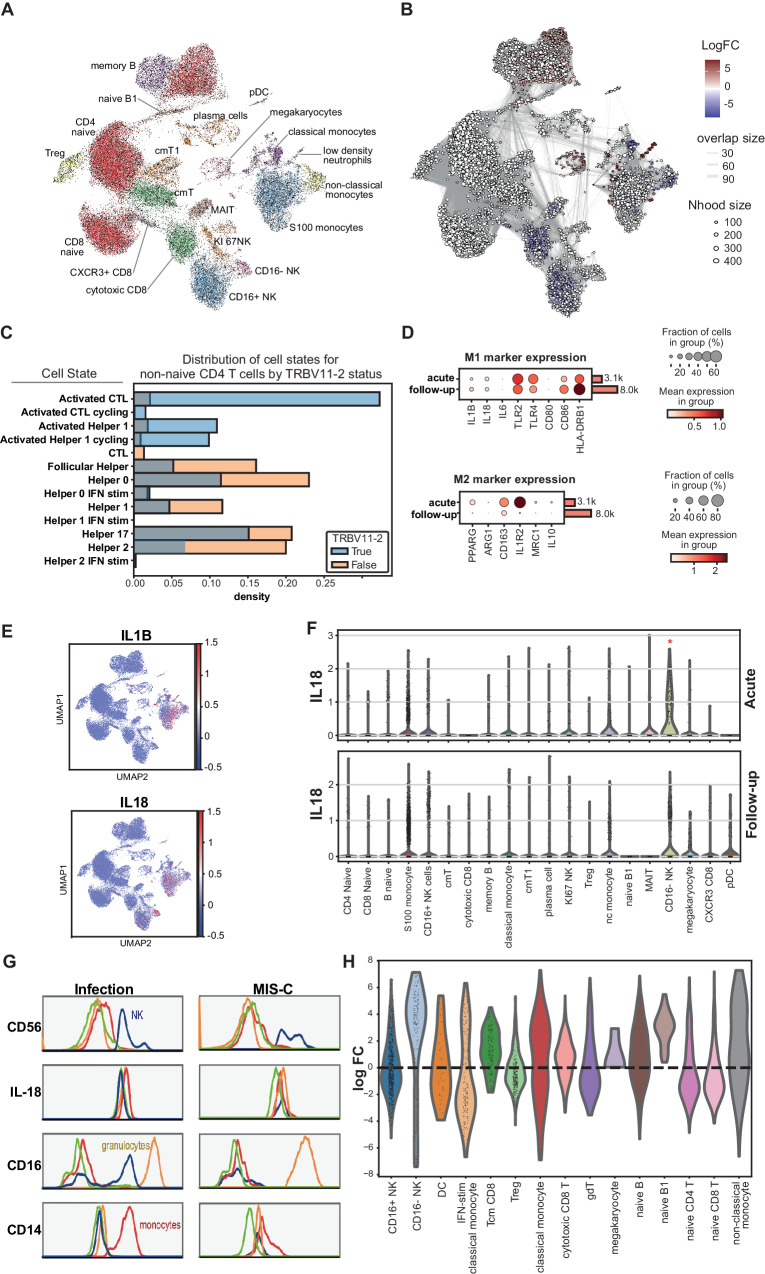
Multisystem inflammatory syndrome in children is a post-infectious presentation SARS-CoV-2 associated with expansion of the T cell receptor Vβ21.3+ T-cell subgroup. Here we apply muti-single cell omics to compare the inflammatory process in children with acute respiratory COVID-19 and those presenting with non SARS-CoV-2 infections in children. Here we show that in Multi-Inflammatory Syndrome in Children (MIS-C), the natural killer cell and monocyte population demonstrate heightened CD95 (Fas) and Interleuking 18 receptor expression. Additionally, TCR Vβ21.3+ CD4+ T-cells exhibit skewed differentiation towards T helper 1, 17 and regulatory T cells, with increased expression of the co-stimulation receptors ICOS, CD28 and interleukin 18 receptor. We observe no functional evidence for NLRP3 inflammasome pathway overactivation, though MIS-C monocytes show elevated active caspase 8. This, coupled with raised IL18 mRNA expression in CD16- NK cells on single cell RNA sequencing analysis, suggests interleukin 18 and CD95 signalling may trigger activation of TCR Vβ21.3+ T-cells in MIS-C, driven by increased IL-18 production from activated monocytes and CD16- Natural Killer cells.
© 2024. The Author(s).
Conflict of interest statement
In the past three years, S.A.T. has received remuneration for Scientific Advisory Board Membership from Sanofi, GlaxoSmithKline, Foresite Labs and Qiagen. S.A.T. is a co-founder and holds equity in Transition Bio. C.E.B. is on the SAB of NodThera, Lightcast, Related Sciences and Janssen Pharmaceuticals and is a co-founder of Polypharmakos and Danger Bio. N.P. received an honorarium from Biomerieux Diagnostics. The other authors declare no competing interests.
Figures
Similar articles
-
Polyclonal expansion of TCR Vbeta 21.3+ CD4+ and CD8+ T cells is a hallmark of Multisystem Inflammatory Syndrome in Children.Sci Immunol. 2021 May 25;6(59):eabh1516. doi: 10.1126/sciimmunol.abh1516. Sci Immunol. 2021. PMID: 34035116 Free PMC article.
-
TIM3+ TRBV11-2 T cells and IFNγ signature in patrolling monocytes and CD16+ NK cells delineate MIS-C.J Exp Med. 2022 Feb 7;219(2):e20211381. doi: 10.1084/jem.20211381. Epub 2021 Dec 16. J Exp Med. 2022. PMID: 34914824 Free PMC article.
-
Upregulation of type 1 conventional dendritic cells implicates antigen cross-presentation in multisystem inflammatory syndrome.J Allergy Clin Immunol. 2022 Mar;149(3):912-922. doi: 10.1016/j.jaci.2021.10.015. Epub 2021 Oct 22. J Allergy Clin Immunol. 2022. PMID: 34688775 Free PMC article.
-
Genetic and Epigenetic Regulation of the Innate Immune Response to Gout.Immunol Invest. 2023 Apr;52(3):364-397. doi: 10.1080/08820139.2023.2168554. Epub 2023 Feb 6. Immunol Invest. 2023. PMID: 36745138 Review.
-
Phenotype, Susceptibility, Autoimmunity, and Immunotherapy Between Kawasaki Disease and Coronavirus Disease-19 Associated Multisystem Inflammatory Syndrome in Children.Front Immunol. 2021 Feb 26;12:632890. doi: 10.3389/fimmu.2021.632890. eCollection 2021. Front Immunol. 2021. PMID: 33732254 Free PMC article.
Cited by
-
SARS-CoV-2 spike does not interact with the T cell receptor or directly activate T cells.Proc Natl Acad Sci U S A. 2024 Jul 30;121(31):e2406615121. doi: 10.1073/pnas.2406615121. Epub 2024 Jul 23. Proc Natl Acad Sci U S A. 2024. PMID: 39042676 Free PMC article.
-
Distinct type 1 immune networks underlie the severity of restrictive lung disease after COVID-19.Nat Immunol. 2025 Apr;26(4):595-606. doi: 10.1038/s41590-025-02110-0. Epub 2025 Mar 26. Nat Immunol. 2025. PMID: 40140496
-
Identification of potential drug targets for achalasia from genetic insights: a Mendelian randomization study.J Cardiothorac Surg. 2025 Jul 14;20(1):296. doi: 10.1186/s13019-025-03538-z. J Cardiothorac Surg. 2025. PMID: 40653474 Free PMC article.
References
MeSH terms
Substances
Supplementary concepts
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
