

The Effect of Neoadjuvant Systemic Therapy on Surgical Outcomes After Lymph Node Dissections for Stage III Melanoma; An Australian Cohort
- PMID: 38762644
- PMCID: PMC11236868
- DOI: 10.1245/s10434-024-15274-0
The Effect of Neoadjuvant Systemic Therapy on Surgical Outcomes After Lymph Node Dissections for Stage III Melanoma; An Australian Cohort
Abstract
Background: Neoadjuvant systemic therapy (NAST) for patients with stage III melanoma achieves high major pathologic response rates and high recurrence-free survival rates. This study aimed to determine how NAST with targeted therapies (TTs) and immune checkpoint inhibitors (ICIs) influences surgical outcomes after lymph node dissection in terms of complications, morbidity, and textbook outcomes.
Methods: Patients who underwent a lymph node dissection after either NAST in a clinical trial or upfront surgery for stage III melanoma between 2014 and 2022 were identified from an institutional research database.
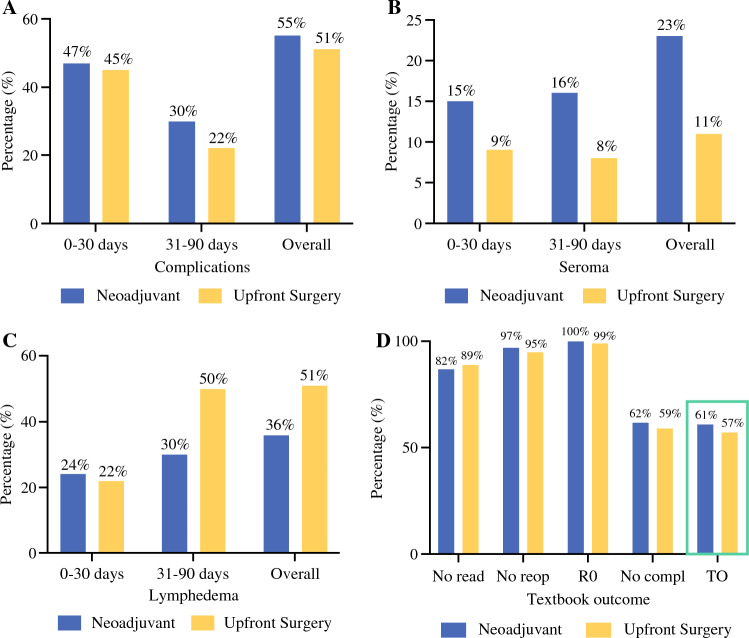
Results: The study included 89 NAST-treated patients and 79 upfront surgery-treated patients. The rate of postoperative complications did not differ between the NAST- and upfront surgery-treated patients (55% vs. 51%; p = 0.643), and steroid treatment for drug toxicity did not influence the complication rate (odds ratio [OR], 1.1; 95% confidence interval [CI], 0.4-3; p = 0.826). No significant differences in postoperative morbidity were observed in terms of seroma (23% vs. 11%; p = 0.570) or lymphedema (36% vs. 51%; p = 0.550). The rate of achieving a textbook outcome was comparable for the two groups (61% vs. 57%; p = 0.641).
Conclusions: The surgical outcomes after lymph node dissections were comparable between the patients who received NAST and those who had upfront surgery, indicating that surgery can be safely performed after NAST with TT or ICI for stage III melanoma.
Keywords: Complications; Melanoma; Neoadjuvant; Surgery; Systemic therapy; Textbook outcomes.
© 2024. The Author(s).
Conflict of interest statement
Alexander M. Menzies has served on an advisory board for BMS, MSD, Novartis, Roche, Pierre-Fabre, and QBiotics. John F. Thompson has received honoraria for advisory board participation from BMS Australia, MSD Australia, GSK, and Provectus Biopharmaceuticals Inc, and travel and conference support from GSK, Provectus Inc, and Novartis. Richard A. Scolyer has received fees for professional services from MetaOptima Technology Inc., F. Hoffmann-La Roche Ltd, Evaxion, Provectus Biopharmaceuticals Australia, Qbiotics, Novartis, Merck Sharp & Dohme, NeraCare, AMGEN Inc., Bristol-Myers Squibb, Myriad Genetics, and GlaxoSmithKline. Robyn P. M. Sawhas received honoraria for advisory board participation from MSD, Novartis, and Qbiotics, and speaking honoraria from BMS and Novartis. Robert V. Rawson has received honoraria for speaking and advisory board participation from Merck Sharp & Dohme. Georgina V. Long is consultant advisor for Agenus, Amgen, Array Biopharma, AstraZeneca, Boehringer Ingelheim, Bristol Myers Squibb, Evaxion, Hexal AG (Sandoz Company), Highlight Therapeutics S.L., Innovent Biologics USA, Merck Sharpe & Dohme, Novartis, PHMR Ltd, Pierre Fabre, Provectus, Qbiotics, and Regeneron. Alexander C. J. van Akkooi declares advisory board and consultancy honoraria at Amgen, Bristol-Myers Squibb, MSD-Merck, Merck-Pfizer, Neracare, Novartis, Pierre Fabre, Sanofi, and Sirius Medical, 4SC, and research grants from Amgen and Merck-Pfizer. The remaining authors have no conflicts of interest.
Figures
Similar articles
-
Surgical outcomes of lymph node dissections for stage III melanoma after neoadjuvant systemic therapy are not inferior to upfront surgery.Eur J Cancer. 2023 May;185:131-138. doi: 10.1016/j.ejca.2023.03.003. Epub 2023 Mar 7. Eur J Cancer. 2023. PMID: 36989829
-
Impact of personalized response-directed surgery and adjuvant therapy on survival after neoadjuvant immunotherapy in stage III melanoma: Comparison of 3-year data from PRADO and OpACIN-neo.Eur J Cancer. 2025 Jan;214:115141. doi: 10.1016/j.ejca.2024.115141. Epub 2024 Nov 19. Eur J Cancer. 2025. PMID: 39602990 Clinical Trial.
-
Neoadjuvant plus adjuvant dabrafenib and trametinib versus standard of care in patients with high-risk, surgically resectable melanoma: a single-centre, open-label, randomised, phase 2 trial.Lancet Oncol. 2018 Feb;19(2):181-193. doi: 10.1016/S1470-2045(18)30015-9. Epub 2018 Jan 18. Lancet Oncol. 2018. PMID: 29361468 Clinical Trial.
-
Adjuvant therapy of malignant melanoma and the role of sentinel node mapping.Recent Results Cancer Res. 2000;157:178-89. doi: 10.1007/978-3-642-57151-0_15. Recent Results Cancer Res. 2000. PMID: 10857171 Review.
-
The Landmark Series: Neoadjuvant Systemic Therapy (NAST) for Stage 3 Melanoma Patients - A Potential Paradigm Shift in Management.Ann Surg Oncol. 2020 Jul;27(7):2188-2200. doi: 10.1245/s10434-020-08566-8. Epub 2020 May 14. Ann Surg Oncol. 2020. PMID: 32409966 Review.
Cited by
-
Investigating the potential of oncolytic viruses in the treatment of melanoma: where do we go from here?Skin Health Dis. 2025 Apr 22;5(2):102-113. doi: 10.1093/skinhd/vzaf022. eCollection 2025 Apr. Skin Health Dis. 2025. PMID: 40365251 Free PMC article. Review.
References
-
- Liu J, Blake SJ, Yong MCR, et al. Improved efficacy of neoadjuvant compared to adjuvant immunotherapy to eradicate metastatic disease. Cancer Discov. 2016;6:1382–1399. doi: 10.1158/2159-8290.Cd-16-0577. - DOI - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
