

Bisoprolol in Patients With Chronic Obstructive Pulmonary Disease at High Risk of Exacerbation: The BICS Randomized Clinical Trial
- PMID: 38762800
- PMCID: PMC11322848
- DOI: 10.1001/jama.2024.8771
Bisoprolol in Patients With Chronic Obstructive Pulmonary Disease at High Risk of Exacerbation: The BICS Randomized Clinical Trial
Abstract
Importance: Chronic obstructive pulmonary disease (COPD) is a leading cause of morbidity and mortality worldwide. Observational studies report that β-blocker use may be associated with reduced risk of COPD exacerbations. However, a recent trial reported that metoprolol did not reduce COPD exacerbations and increased COPD exacerbations requiring hospital admission.
Objective: To test whether bisoprolol decreased COPD exacerbations in people with COPD at high risk of exacerbations.
Design, setting, and participants: The Bisoprolol in COPD Study (BICS) was a double-blind placebo-controlled randomized clinical trial conducted in 76 UK sites (45 primary care clinics and 31 secondary clinics). Patients with COPD who had at least moderate airflow obstruction on spirometry (ratio of forced expiratory volume in the first second of expiration [FEV1] to forced vital capacity <0.7; FEV1 <80% predicted) and at least 2 COPD exacerbations treated with oral corticosteroids, antibiotics, or both in the prior 12 months were enrolled from October 17, 2018, to May 31, 2022. Follow-up concluded on April 18, 2023.
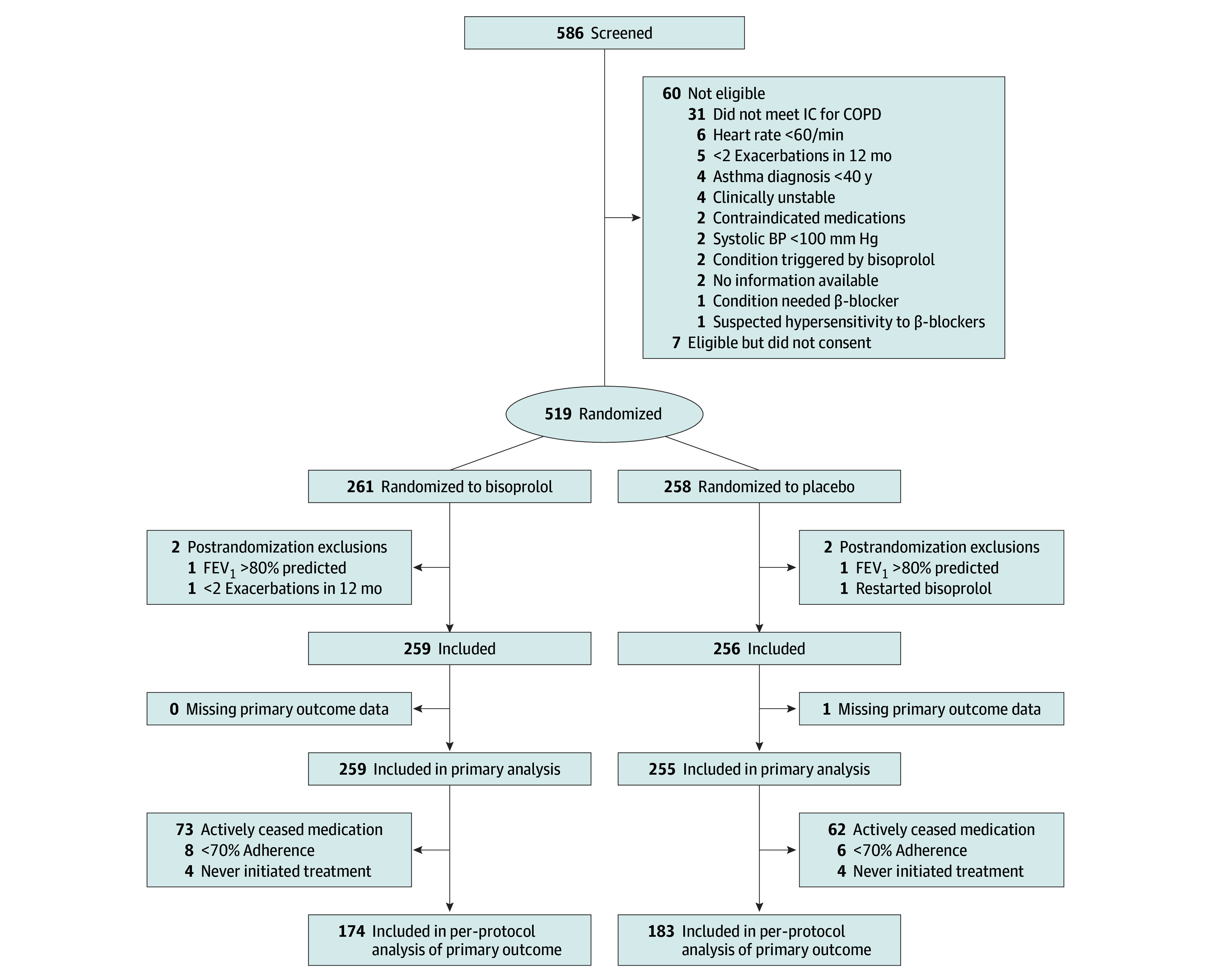
Interventions: Patients were randomly assigned to bisoprolol (n = 261) or placebo (n = 258). Bisoprolol was started at 1.25 mg orally daily and was titrated as tolerated during 4 sessions to a maximum dose of 5 mg/d, using a standardized protocol.
Main outcomes and measures: The primary clinical outcome was the number of patient-reported COPD exacerbations treated with oral corticosteroids, antibiotics, or both during the 1-year treatment period. Safety outcomes included serious adverse events and adverse reactions.
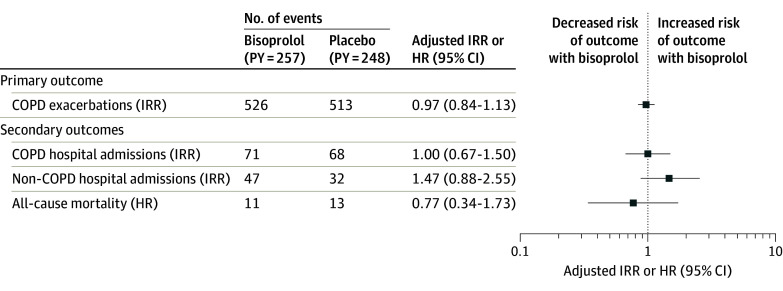
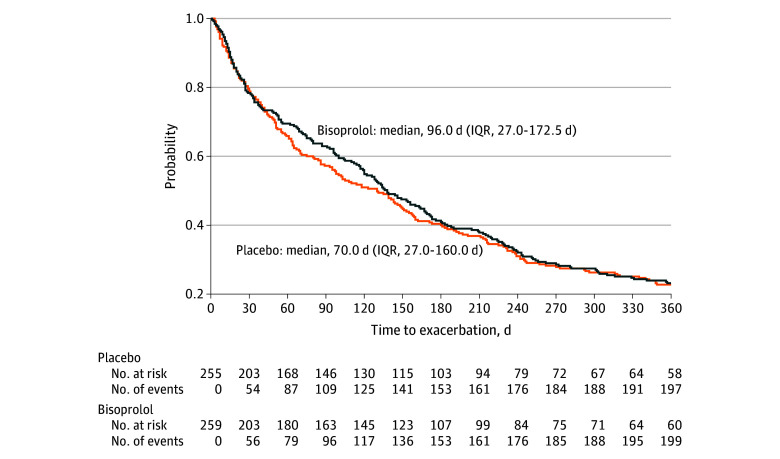
Results: Although the trial planned to enroll 1574 patients, recruitment was suspended from March 16, 2020, to July 31, 2021, due to the COVID-19 pandemic. Two patients in each group were excluded postrandomization. Among the 515 patients (mean [SD] age, 68 [7.9] years; 274 men [53%]; mean FEV1, 50.1%), primary outcome data were available for 514 patients (99.8%) and 371 (72.0%) continued taking the study drug. The primary outcome of patient-reported COPD exacerbations treated with oral corticosteroids, antibiotics, or both was 526 in the bisoprolol group, with a mean exacerbation rate of 2.03/y, vs 513 exacerbations in the placebo group, with a mean exacerbation rate of 2.01/y. The adjusted incidence rate ratio was 0.97 (95% CI, 0.84-1.13; P = .72). Serious adverse events occurred in 37 of 255 patients in the bisoprolol group (14.5%) vs 36 of 251 in the placebo group (14.3%; relative risk, 1.01; 95% CI, 0.62-1.66; P = .96).
Conclusions and relevance: Among people with COPD at high risk of exacerbation, treatment with bisoprolol did not reduce the number of self-reported COPD exacerbations requiring treatment with oral corticosteroids, antibiotics, or both.
Trial registration: isrctn.org Identifier: ISRCTN10497306.
Conflict of interest statement
Figures
Comment in
-
β-Blockers in Chronic Obstructive Pulmonary Disease-Walking the Tightrope.JAMA. 2024 Aug 13;332(6):458-459. doi: 10.1001/jama.2024.8743. JAMA. 2024. PMID: 38762796 No abstract available.
References
-
- World Health Organization . The top 10 causes of death. Published December 9, 2020. Accessed April 30, 2024. https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
