

Intra thyroid thymic carcinoma: A case report and literature review
- PMID: 38762961
- PMCID: PMC11126938
- DOI: 10.1016/j.ijscr.2024.109762
Intra thyroid thymic carcinoma: A case report and literature review
Abstract
Introduction and importance: Intrathyroid thymic carcinoma (ITC) is a malignant epithelial tumor with thymic differentiation within the thyroid gland. Its frequency is up to 0.15 % of all malignant thyroid tumors. It is frequently a low-grade tumor. The clinical status is often misleading to other more advanced tumors like cervical lymph node metastasis of nonkeratinizing squamous cell carcinoma, undifferentiated variant, dedifferentiated carcinoma, and medullary carcinoma of the thyroid.
Case preparation: The patient came to us with the diagnosis of cervical lymph node metastasis of undifferentiated carcinoma. This patient was first diagnosed with cervical lymph node metastasis in the previous hospital. After having an ITC diagnosis, the patient was operated on the rennet of thyroid glands and had a low dose of radio-chemotherapy for recurrent prevention purposes. It is the first case of such a disease diagnosed at our hospital and also the first case reported in Vietnam.
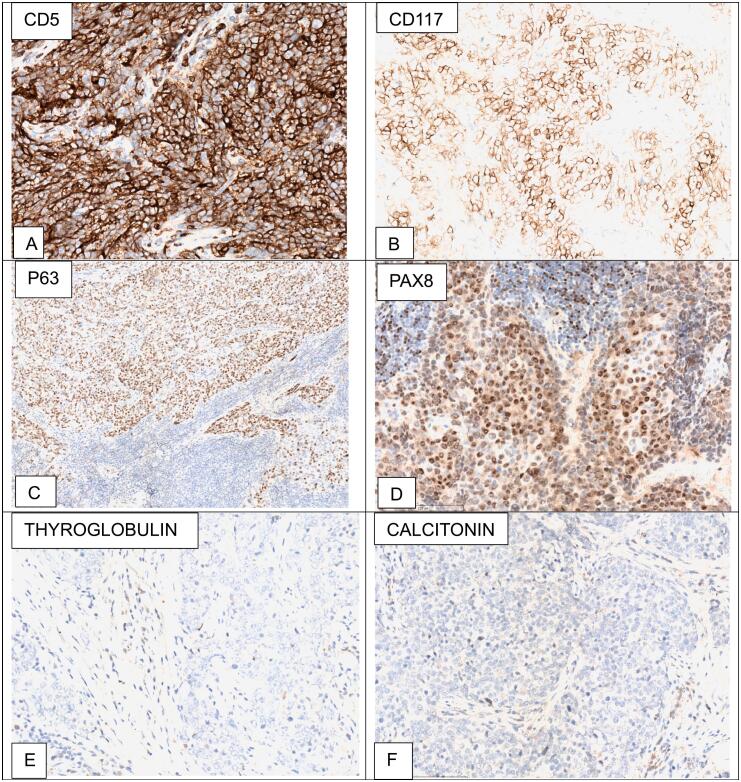
Clinical discussion: ITC is rare and appears similar to all thymic carcinoma variants. The most popular type is squamous carcinoma. Immunohistochemical stains are typical for thymic origin tumors with CD5, CD117 positive. ITC is often negative for monoclonal PAX8 but positive in this case (MRQ-50 clone, Sigma-Aldrich). This finding is an exciting one that should considered.
Conclusion: Reporting the case increases the awareness of the disease, especially among Vietnam Doctors and patients.
Keywords: Case report; Intrathyroid thymic carcinoma; Thyroid cancers.
Copyright © 2024 The Authors. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of competing interest The authors declare no potential conflicts of interest concerning this article's research, authorship, and publication.
Figures


Similar articles
-
[Clinicopathological Features of Intrathyroid Thymic Carcinoma].Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2021 Feb 28;43(1):42-46. doi: 10.3881/j.issn.1000-503X.12609. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2021. PMID: 33663661 Chinese.
-
Intrathyroid epithelial thymoma (ITET) and carcinoma showing thymus-like differentiation (CASTLE): CD5-positive neoplasms mimicking squamous cell carcinoma of the thyroid.Histol Histopathol. 2013 May;28(5):543-56. doi: 10.14670/HH-28.543. Epub 2012 Dec 11. Histol Histopathol. 2013. PMID: 23233417
-
[A Case of Carcinoma Showing Thymus-Like Differentiation (CASTLE) of the Thyroid].J UOEH. 2018;40(3):259-266. doi: 10.7888/juoeh.40.259. J UOEH. 2018. PMID: 30224623 Japanese.
-
Intrasalivary Thymic Carcinoma: A Case Report and Literature Review.Head Neck Pathol. 2022 Sep;16(3):857-864. doi: 10.1007/s12105-021-01394-6. Epub 2021 Nov 22. Head Neck Pathol. 2022. PMID: 34807356 Free PMC article. Review.
-
Overview of the 2022 WHO Classification of Thyroid Neoplasms.Endocr Pathol. 2022 Mar;33(1):27-63. doi: 10.1007/s12022-022-09707-3. Epub 2022 Mar 14. Endocr Pathol. 2022. PMID: 35288841 Review.
References
-
- Collins J.A., Ping B., Bishop J.A., Ali S.Z. Carcinoma showing thymus-like differentiation (CASTLE): cytopathological features and differential diagnosis. Acta Cytol. 2016;60(5):421–428. - PubMed
-
- Reimann J.D., Dorfman D.M., Nosé V. Carcinoma showing thymus-like differentiation of the thyroid (CASTLE): a comparative study: evidence of thymic differentiation and solid cell nest origin. Am. J. Surg. Pathol. 2006;30(8):994–1001. - PubMed
-
- Baloch Z., Cameselle-Teijeiro A.S. WHO Classification of Tumours Editorial Board. Endocrine and neuroendocrine tumours [Internet]. WHO Classification of Tumours Editorial Board Endocrine and neuroendocrine tumours [Internet] 5th ed. International Agency for Research on Cancer; 2022. Thyroid tumours.https://tumourclassification.iarc.who.int/chapters/53
Publication types
LinkOut - more resources
Full Text Sources
