

Duration of androgen deprivation therapy with postoperative radiotherapy for prostate cancer: a comparison of long-course versus short-course androgen deprivation therapy in the RADICALS-HD randomised trial
- PMID: 38763153
- PMCID: PMC7616389
- DOI: 10.1016/S0140-6736(24)00549-X
Duration of androgen deprivation therapy with postoperative radiotherapy for prostate cancer: a comparison of long-course versus short-course androgen deprivation therapy in the RADICALS-HD randomised trial
Abstract
Background: Previous evidence supports androgen deprivation therapy (ADT) with primary radiotherapy as initial treatment for intermediate-risk and high-risk localised prostate cancer. However, the use and optimal duration of ADT with postoperative radiotherapy after radical prostatectomy remains uncertain.
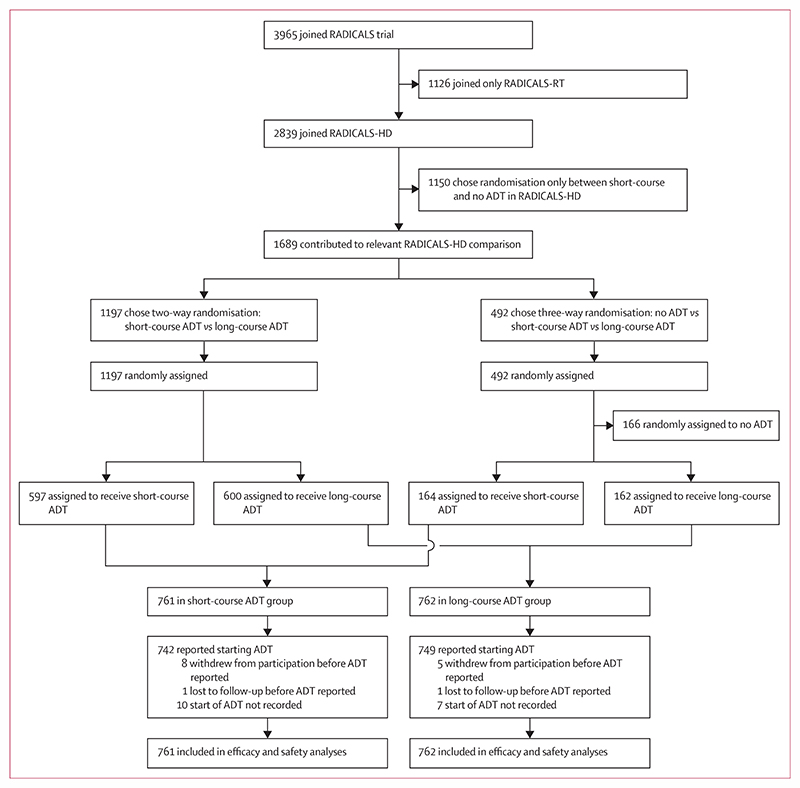
Methods: RADICALS-HD was a randomised controlled trial of ADT duration within the RADICALS protocol. Here, we report on the comparison of short-course versus long-course ADT. Key eligibility criteria were indication for radiotherapy after previous radical prostatectomy for prostate cancer, prostate-specific antigen less than 5 ng/mL, absence of metastatic disease, and written consent. Participants were randomly assigned (1:1) to add 6 months of ADT (short-course ADT) or 24 months of ADT (long-course ADT) to radiotherapy, using subcutaneous gonadotrophin-releasing hormone analogue (monthly in the short-course ADT group and 3-monthly in the long-course ADT group), daily oral bicalutamide monotherapy 150 mg, or monthly subcutaneous degarelix. Randomisation was done centrally through minimisation with a random element, stratified by Gleason score, positive margins, radiotherapy timing, planned radiotherapy schedule, and planned type of ADT, in a computerised system. The allocated treatment was not masked. The primary outcome measure was metastasis-free survival, defined as metastasis arising from prostate cancer or death from any cause. The comparison had more than 80% power with two-sided α of 5% to detect an absolute increase in 10-year metastasis-free survival from 75% to 81% (hazard ratio [HR] 0·72). Standard time-to-event analyses were used. Analyses followed intention-to-treat principle. The trial is registered with the ISRCTN registry, ISRCTN40814031, and ClinicalTrials.gov, NCT00541047.
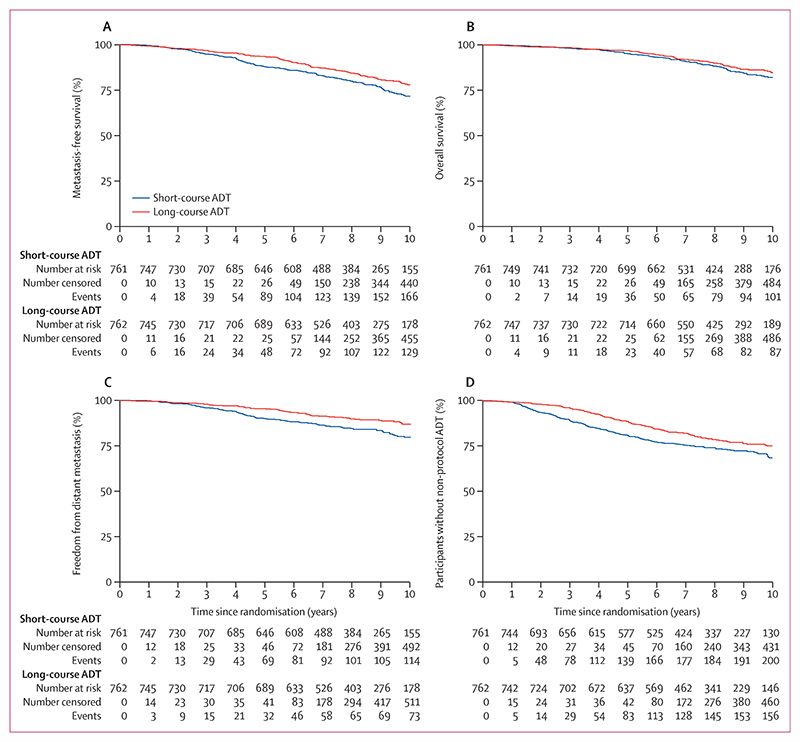
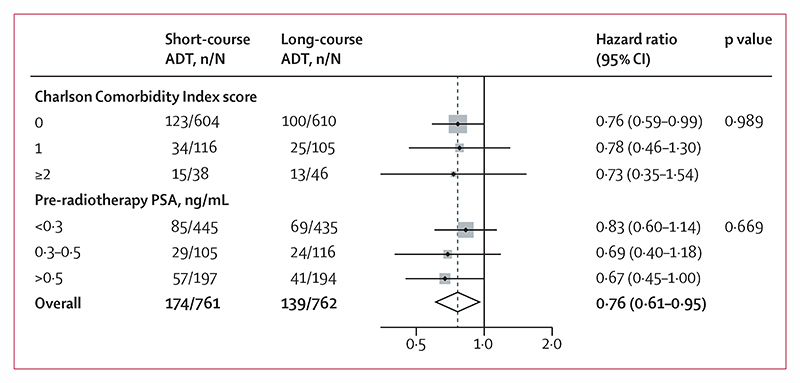
Findings: Between Jan 30, 2008, and July 7, 2015, 1523 patients (median age 65 years, IQR 60-69) were randomly assigned to receive short-course ADT (n=761) or long-course ADT (n=762) in addition to postoperative radiotherapy at 138 centres in Canada, Denmark, Ireland, and the UK. With a median follow-up of 8·9 years (7·0-10·0), 313 metastasis-free survival events were reported overall (174 in the short-course ADT group and 139 in the long-course ADT group; HR 0·773 [95% CI 0·612-0·975]; p=0·029). 10-year metastasis-free survival was 71·9% (95% CI 67·6-75·7) in the short-course ADT group and 78·1% (74·2-81·5) in the long-course ADT group. Toxicity of grade 3 or higher was reported for 105 (14%) of 753 participants in the short-course ADT group and 142 (19%) of 757 participants in the long-course ADT group (p=0·025), with no treatment-related deaths.
Interpretation: Compared with adding 6 months of ADT, adding 24 months of ADT improved metastasis-free survival in people receiving postoperative radiotherapy. For individuals who can accept the additional duration of adverse effects, long-course ADT should be offered with postoperative radiotherapy.
Funding: Cancer Research UK, UK Research and Innovation (formerly Medical Research Council), and Canadian Cancer Society.
Copyright © 2024 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Declaration of interests AN reports honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Merck. ADC reports research grants for the STAMPEDE trial from Janssen, Astellas, Novartis, Sanofi, and Clovis. CMH is an executive committee member for the British Uro-Oncology Group. CNC reports support for the present manuscript from the Canadian Cancer Trials Group; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Bayer Corp, Knight Therapeutics, and AbbVie. CLG reports that they participate in the independent data monitoring and steering committee for the BARCODE study at the Institute of Cancer Research in London (principal investigator Ros Eeles). CB reports stock or stock options from GSK; and has been an employee at GSK since August, 2023. CCP reports consulting fees from AAA, ITM Radiopharma, Myovant, and Clarity Pharmaceuticals to his institution; and payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Janssen and Bayer to his institution. FS reports grants or contracts from Janssen, Bayer, Merck, Pfizer, Astellas, Bristol Myers Squibb (BMS), Novartis, Sanofi, and AstraZeneca to his institution; consulting fees from Janssen, Bayer, Astellas, BMS, Novartis, Sanofi, AstraZeneca, Merck, and Pfizer to him; and payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Janssen, Bayer, Myovant, Astellas, BMS, Novartis, Sanofi, AstraZeneca, Merck, and Pfizer to him. LCB reports that their previous Institute of Cancer role was funded in part by a Biomedical Research Centre grant which was paid to the institution; the role was not connected to the RADICALS trial. MRS reports research grants and biomarker testing costs, all to institution and all active in past 36 months but on research outside of this research, from Astellas, Clovis Oncology, Janssen, Novartis, and Sanofi-Aventis; consulting fees from Eli Lilly; speaker fees at a clinical trial statistics training meeting for clinicians (no discussion of particular drugs) from Lilly Oncology, Janssen, and Eisai; and is an independent member of many independent data monitoring committees but all for academic sponsors and unpaid. NDJ is a Senior Investigator for the National Institute for Health and Care Research. NWC reports honoraria for lectures, advisory boards, and symposia from AstraZeneca, Janssen, Bayer, and Pfizer; support for travel to and attendance at a European meeting from Bayer; participation on an independent data monitoring committee for the Probio trial (Karolinska), and the trial steering committee for the Capi 28 Trial (AstraZeneca) and the STAMPEDE Trial (Medical Research Council [MRC]); and is the Joint National Clinical Lead for National Prostate Cancer Audit. PW reports an educational event payment from Astellas; conference and travel cost support from AstraZeneca and Aventis; and participation on the advisory board for Ferring and Roche. PWMC reports grants or contracts from CARO-ACURA and the Canadian Institutes of Health Research; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Pfizer and EMD Serono; and participation on a data safety monitoring board or advisory board for TerSera, AbbVie, Tolmar, and Knight Therapeutics. PMP reports participation on a data safety monitoring board or advisory board for AAA Nordic, MSD, and Pfizer Denmark. SCM reports honoraria from Janssen, Astellas, Knight Therapeutics, Amgen Pharmaceutical, AstraZeneca, AbbVie, and Bayer; and support for attending meetings or travel from TerSera and Sanofi. WRC reports consulting fees from Bayer and Janssen; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Astellas, Bayer, Janssen, AAA Novartis, and Myriad Genetics; and support for attending meetings or travel from Janssen, AAA Novartis, and Bayer. All other authors declare no competing interests.
Figures
Comment in
-
Androgen deprivation therapy combined with postoperative radiotherapy for prostate cancer management.Lancet. 2024 Jun 1;403(10442):2353-2355. doi: 10.1016/S0140-6736(24)00802-X. Epub 2024 May 16. Lancet. 2024. PMID: 38763152 No abstract available.
References
-
- Kishan AU, Sun Y, Hartman H, et al. Androgen deprivation therapy use and duration with definitive radiotherapy for localised prostate cancer: an individual patient data meta-analysis. Lancet Oncol. 2022;23:304–16. - PubMed
-
- Carrie C, Magné N, Burban-Provost P, et al. Short-term androgen deprivation therapy combined with radiotherapy as salvage treatment after radical prostatectomy for prostate cancer (GETUG-AFU 16): a 112-month follow-up of a phase 3, randomised trial. Lancet Oncol. 2019;20:1740–49. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
