

Optimization and impact of sensitivity mode on abbreviated scan protocols with population-based input function for parametric imaging of [18F]-FDG for a long axial FOV PET scanner
- PMID: 38763962
- PMCID: PMC11368996
- DOI: 10.1007/s00259-024-06745-3
Optimization and impact of sensitivity mode on abbreviated scan protocols with population-based input function for parametric imaging of [18F]-FDG for a long axial FOV PET scanner
Abstract
Background: The long axial field of view, combined with the high sensitivity of the Biograph Vision Quadra PET/CT scanner enables the precise deviation of an image derived input function (IDIF) required for parametric imaging. Traditionally, this requires an hour-long dynamic PET scan for [18F]-FDG, which can be significantly reduced by using a population-based input function (PBIF). In this study, we expand these examinations and include the scanner's ultra-high sensitivity (UHS) mode in comparison to the high sensitivity (HS) mode and evaluate the potential for further shortening of the scan time.
Methods: Patlak Ki and DV estimates were determined by the indirect and direct Patlak methods using dynamic [18F]-FDG data of 6 oncological patients with 26 lesions (0-65 min p.i.). Both sensitivity modes for different number/duration of PET data frames were compared, together with the potential of using abbreviated scan durations of 20, 15 and 10 min by using a PBIF. The differences in parametric images and tumour-to-background ratio (TBR) due to the shorter scans using the PBIF method and between the sensitivity modes were assessed.
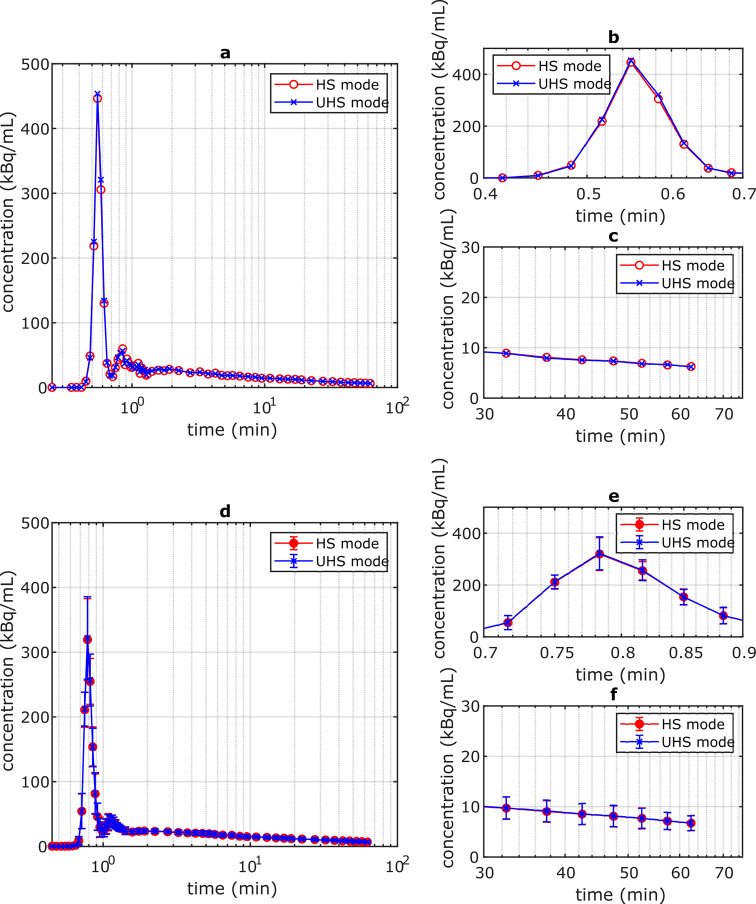
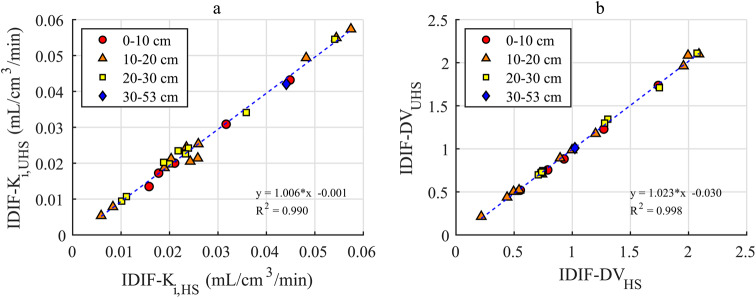
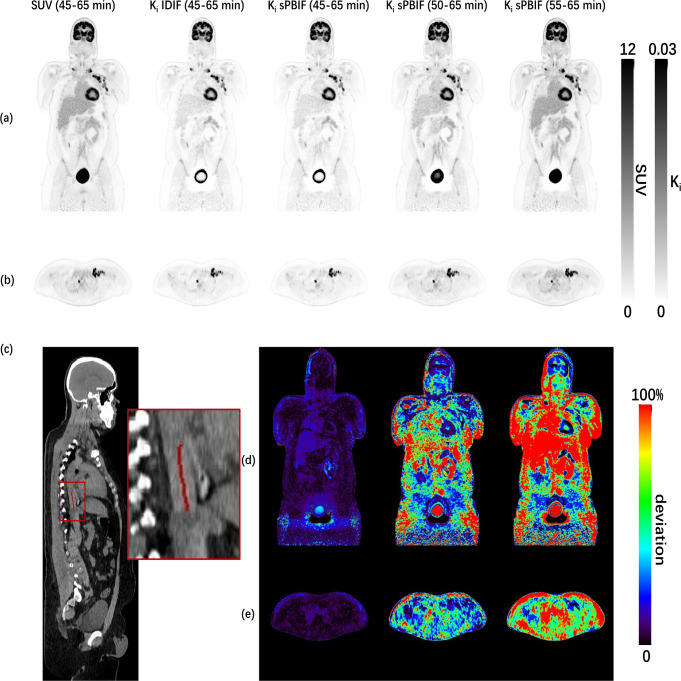
Results: A difference of 3.4 ± 7.0% (Ki) and 1.2 ± 2.6% (DV) was found between both sensitivity modes using indirect Patlak and the full IDIF (0-65 min). For the abbreviated protocols and indirect Patlak, the UHS mode resulted in a lower bias and higher precision, e.g., 45-65 min p.i. 3.8 ± 4.4% (UHS) and 6.4 ± 8.9% (HS), allowing shorter scan protocols, e.g. 50-65 min p.i. 4.4 ± 11.2% (UHS) instead of 7.3 ± 20.0% (HS). The variation of Ki and DV estimates for both Patlak methods was comparable, e.g., UHS mode 3.8 ± 4.4% and 2.7 ± 3.4% (Ki) and 14.4 ± 2.7% and 18.1 ± 7.5% (DV) for indirect and direct Patlak, respectively. Only a minor impact of the number of Patlak frames was observed for both sensitivity modes and Patlak methods. The TBR obtained with direct Patlak and PBIF was not affected by the sensitivity mode, was higher than that derived from the SUV image (6.2 ± 3.1) and degraded from 20.2 ± 12.0 (20 min) to 10.6 ± 5.4 (15 min). Ki and DV estimate images showed good agreement (UHS mode, RC: 6.9 ± 2.3% (Ki), 0.1 ± 3.1% (DV), peak signal-to-noise ratio (PSNR): 64.5 ± 3.3 dB (Ki), 61.2 ± 10.6 dB (DV)) even for abbreviated scan protocols of 50-65 min p.i.
Conclusions: Both sensitivity modes provide comparable results for the full 65 min dynamic scans and abbreviated scans using the direct Patlak reconstruction method, with good Ki and DV estimates for 15 min short scans. For the indirect Patlak approach the UHS mode improved the Ki estimates for the abbreviated scans.
Keywords: LAFOV PET; Parametric imaging; Patlak; Population-based input function; Total-body PET.
© 2024. The Author(s).
Conflict of interest statement
Hasan Sari is a full-time employee of Siemens Healthineers. Fabian P. Schmidt and Christian la Fougère received a research grant from Siemens Healthineers. Axel Rominger has received research support and speaker honoraria from Siemens Healthineers. There are no other conflicts of interest to report.
Figures




Similar articles
-
Feasibility of using abbreviated scan protocols with population-based input functions for accurate kinetic modeling of [18F]-FDG datasets from a long axial FOV PET scanner.Eur J Nucl Med Mol Imaging. 2023 Jan;50(2):257-265. doi: 10.1007/s00259-022-05983-7. Epub 2022 Oct 4. Eur J Nucl Med Mol Imaging. 2023. PMID: 36192468 Free PMC article.
-
Impact of different parametric Patlak imaging approaches and comparison with a 2-tissue compartment pharmacokinetic model with a long axial field-of-view (LAFOV) PET/CT in oncological patients.Eur J Nucl Med Mol Imaging. 2025 Jan;52(2):623-637. doi: 10.1007/s00259-024-06879-4. Epub 2024 Sep 11. Eur J Nucl Med Mol Imaging. 2025. PMID: 39256215 Free PMC article.
-
Ultrashort Oncologic Whole-Body [18F]FDG Patlak Imaging Using LAFOV PET.J Nucl Med. 2024 Oct 1;65(10):1652-1657. doi: 10.2967/jnumed.124.267784. J Nucl Med. 2024. PMID: 39353647
-
Quantitative approaches of dynamic FDG-PET and PET/CT studies (dPET/CT) for the evaluation of oncological patients.Cancer Imaging. 2012 Sep 28;12(1):283-9. doi: 10.1102/1470-7330.2012.0033. Cancer Imaging. 2012. PMID: 23033440 Free PMC article. Review.
-
The impact of long axial field of view (LAFOV) PET on oncologic imaging.Eur J Radiol. 2025 Feb;183:111873. doi: 10.1016/j.ejrad.2024.111873. Epub 2024 Dec 4. Eur J Radiol. 2025. PMID: 39647272 Free PMC article. Review.
Cited by
-
Test-retest repeatability of quantitative organ and tissue uptake using 20-minute dynamic multiparametric whole-body [18F]FDG PET/CT in patients with type 2 diabetes.EJNMMI Res. 2025 May 12;15(1):56. doi: 10.1186/s13550-025-01249-z. EJNMMI Res. 2025. PMID: 40354003 Free PMC article.
-
13N-NH3 myocardial perfusion imaging with reduced scan duration: a feasibility study in the era of total-body PET/CT.EJNMMI Phys. 2025 Mar 4;12(1):18. doi: 10.1186/s40658-025-00729-4. EJNMMI Phys. 2025. PMID: 40032742 Free PMC article.
-
A digital twin of the Biograph Vision Quadra long axial field of view PET/CT: Monte Carlo simulation and image reconstruction framework.EJNMMI Phys. 2025 Mar 31;12(1):31. doi: 10.1186/s40658-025-00738-3. EJNMMI Phys. 2025. PMID: 40163262 Free PMC article.
References
-
- Kitson SL, Cuccurullo V, Ciarmiello A, Salvo D, Mansi L. Clinical applications of Positron Emission Tomography (PET) imaging in Medicine: Oncology, Brain diseases and Cardiology. Curr Radiopharm 2:224–53.
-
- Dias AH, Pedersen MF, Danielsen H, Munk OL, Gormsen LC. Clinical feasibility and impact of fully automated multiparametric PET imaging using direct patlak reconstruction: evaluation of 103 dynamic whole-body 18F-FDG PET/CT scans. Eur J Nucl Med Mol Imaging. 2021;48:837–50. 10.1007/s00259-020-05007-2 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous
