

Ruxolitinib plus standard of care in severe hospitalized adults with severe fever with thrombocytopenia syndrome (SFTS): an exploratory, single-arm trial
- PMID: 38764059
- PMCID: PMC11103999
- DOI: 10.1186/s12916-024-03421-z
Ruxolitinib plus standard of care in severe hospitalized adults with severe fever with thrombocytopenia syndrome (SFTS): an exploratory, single-arm trial
Abstract
Background: Severe fever with thrombocytopenia syndrome (SFTS) is an emerging tick-borne infectious disease, and its morbidity and mortality are increasing. At present, there is no specific therapy available. An exacerbated IFN-I response and cytokine storm are related to the mortality of patients with SFTS. Ruxolitinib is a Janus kinase (JAK) 1/2 inhibitor that can block proinflammatory cytokines and inhibit the type I IFN pathway. We aimed to explore the use of ruxolitinib plus standard of care for severe SFTS.
Methods: We conducted a prospective, single-arm study of severe SFTS. We recruited participants aged 18 years or older who were admitted to the hospital with laboratory-confirmed severe SFTS and whose clinical score exceeded 8 points within 6 days of symptom onset. Participants received oral ruxolitinib (10 mg twice a day) for up to 10 days. The primary endpoint was 28-day overall survival. The secondary endpoints included the proportion of participants who needed intensive care unit (ICU) admission, total cost, changes in neurologic symptoms and clinical laboratory parameters, and adverse events (AEs) within 28 days. A historical control group (HC group, n = 26) who met the upper criteria for inclusion and hospitalized from April 1, 2021, to September 16, 2022, was selected and 1:1 matched for baseline characteristics by propensity score matching.
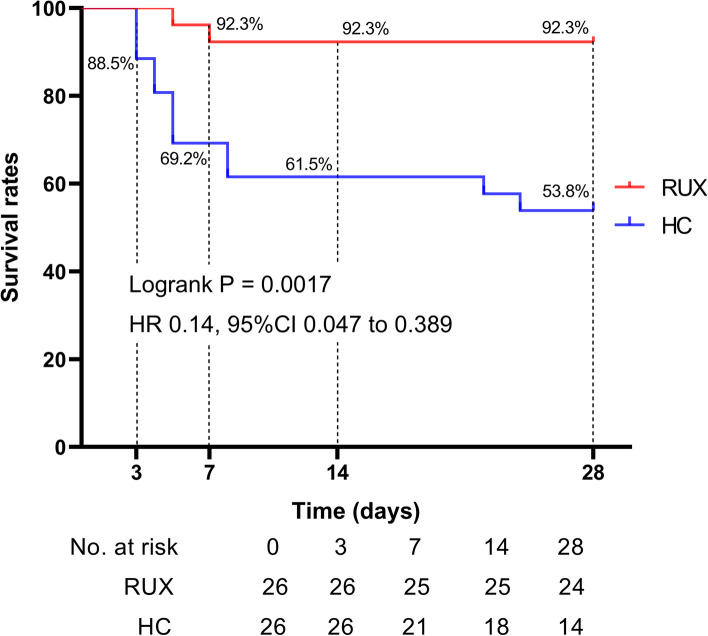
Results: Between Sep 16, 2022, and Sep 16, 2023, 26 participants were recruited into the ruxolitinib treatment group (RUX group). The 28-day overall mortality was 7.7% in the RUX group and 46.2% in the HC group (P = 0.0017). There was a significantly lower proportion of ICU admissions (15.4% vs 65.4%, p < 0.001) and total hospitalization cost in the RUX group. Substantial improvements in neurologic symptoms, platelet counts, hyperferritinemia, and an absolute decrease in the serum SFTS viral load were observed in all surviving participants. Treatment-related adverse events were developed in 6 patients (23.2%) and worsened in 8 patients (30.8%), and no treatment-related serious adverse events were reported.
Conclusions: Our findings indicate that ruxolitinib has the potential to increase the likelihood of survival as well as reduce the proportion of ICU hospitalization and being tolerated in severe SFTS. Further trials are needed.
Trail registration: ChiCTR2200063759, September 16, 2022.
Keywords: Cytokine storm; Ruxolitinib; Severe fever with thrombocytopenia syndrome.
© 2024. The Author(s).
Conflict of interest statement
The authors declare that they have no competing interests.
Figures

References
-
- International Committee on Taxonomy of Viruses. Taxon details: severe fever with thrombocytopenia syndrome virus. [https://ictv.global/taxonomy/taxondetails?taxnode_id=202100166].
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
