

Presentation and management of true aneurysms of the pancreaticoduodenal arcade with concomitant celiac artery stenosis using the endovascular approach
- PMID: 38764461
- PMCID: PMC11099304
- DOI: 10.1016/j.jvscit.2024.101499
Presentation and management of true aneurysms of the pancreaticoduodenal arcade with concomitant celiac artery stenosis using the endovascular approach
Abstract
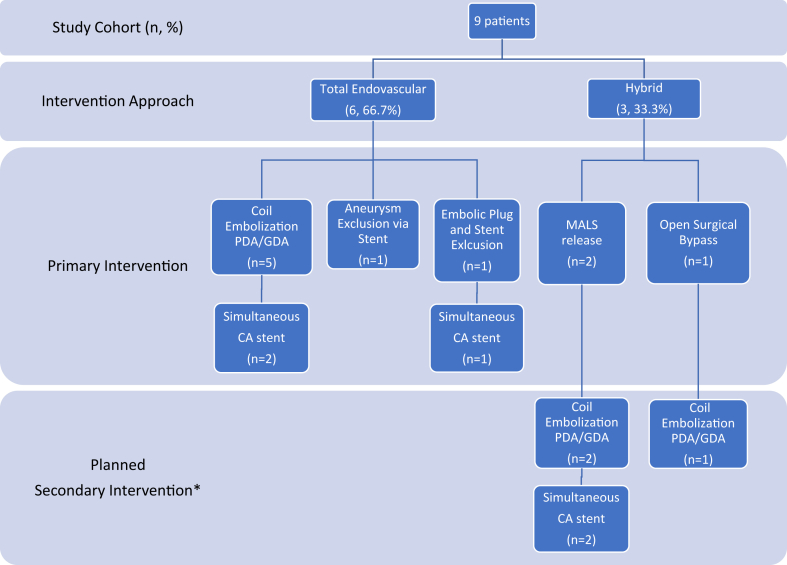
True aneurysms of the pancreaticoduodenal artery (PDA) arcade are rare but require intervention due to the high risk of rupture. Historically, these aneurysms have been managed with open surgical methods. In this study, we describe a contemporary series of aneurysms treated using a modern approach that includes endovascular and hybrid techniques. All the patients with aneurysms of the PDA arcade in an institutional database were identified between 2008 and 2022. Patients with history of pancreatic resection were excluded. Data on demographics, presenting symptoms, imaging findings, operative approach, and outcomes were collected and reviewed. There were nine patients diagnosed with a PDA aneurysm, and all nine underwent endovascular intervention. Most were men (n = 5; 55.6%) and White (n = 7; 77.8%) and had American Society of Anesthesiologists class II or III. The median aneurysm size was 21 mm (range, 6-42 mm), and five (55.5%) were symptomatic. Of the five symptomatic cases, two presented with rupture and were treated urgently. The median time to intervention for the nonurgent cases was 30 days. All but one patient had concomitant celiac artery stenosis and two of the eight cases (25%) were due to extrinsic compression from median arcuate ligament syndrome. Both patients underwent median arcuate ligament syndrome release before endovascular intervention. Another patient required open surgical bypass before endovascular repair from the supraceliac aorta to hepatic artery using a Dacron graft to maintain hepatic perfusion. Among the eight patients with celiac axis stenosis, five (62.5%) required celiac stent placement within the same operation. Coil embolization of the aneurysm was used for all except for two patients (n = 7 of 9; 77.8%), with one patient receiving embolic plugs and another receiving an 8 × 38-mm balloon-expandable covered stent for aneurysm exclusion. The median operating room time was 134 minutes. All repairs were technically successful without any intraoperative or postoperative complications. The mean follow-up was 30 months. There was no morbidity, mortality, or unplanned secondary reinterventions within 6 months after aneurysm repair. Stent patency and aneurysm size remained stable at 2 years of follow-up. True pancreaticoduodenal artery arcade aneurysms can be safely and effectively treated using endovascular and hybrid techniques. Because many of these aneurysms have concomitant celiac artery stenosis, the use of endovascular technology allows for simultaneous treatment of both the aneurysm and the stenosis with exceptional results.
Keywords: Concomitant celiac artery stenosis; Endovascular repair of visceral aneurysms; True pancreaticoduodenal artery arcade aneurysms; Visceral aneurysms.
© 2024 The Authors.
Conflict of interest statement
S.E. is a consultant to Penumbra, Inc. B.D. is an advisor, a consultant, and a speaker to Abbott and Medtronic; and a consultant to Bard and Boston Scientific. The remaining authors report no conflicts.
Figures
References
-
- Tien Y.W., Kao H.L., Wang H.P. Celiac artery stenting: a new strategy for patients with pancreaticoduodenal artery aneurysm associated with stenosis of the celiac artery. J Gastroenterol. 2004;39:81–85. - PubMed
-
- Pasha S.F., Gloviczki P., Stanson A.W., Kamath P.S. Splanchnic artery aneurysms. Mayo Clin Proc. 2007;82:472–479. - PubMed
-
- Katsura M., Gushimiyagi M., Takara H., Mototake H. True aneurysm of the pancreaticoduodenal arteries: a single institution experience. J Gastrointest Surg. 2010;14:1409–1413. - PubMed
-
- Paty P.S.K., Cordero J.A., Clement Darling R., Chang B.B., Shah D.M., Leather R.P. Aneurysms of the pancreaticoduodenal artery. J Vasc Surg. 1996;23:710–713. - PubMed
-
- Granke K., Hollier L.H., Bowen J.C. Pancreaticoduodenal artery aneurysms: changing patterns. South Med J. 1990;83:918–921. - PubMed
LinkOut - more resources
Full Text Sources
