

Cardiogenic pulmonary edema - is it lone cardiogenic? "Missing link" between hemodynamic and other existing mechanisms
- PMID: 38764545
- PMCID: PMC11101961
- DOI: 10.62347/YGQQ8696
Cardiogenic pulmonary edema - is it lone cardiogenic? "Missing link" between hemodynamic and other existing mechanisms
Abstract
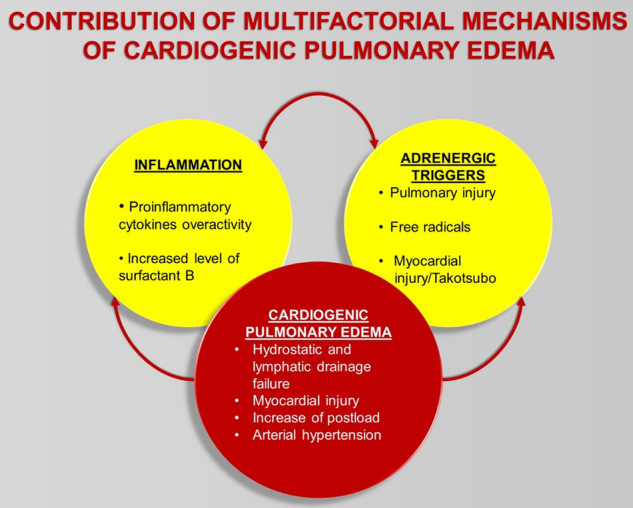
The current traditional pathophysiologic concept of pulmonary edema of cardiogenic origin explains its development by a hydrostatic effect due to increased pulmonary capillary pressure resulting in fluid flux to alveolar and interstitial areas from capillaries. However, several experimental studies and clinical data of poor response to hemodynamic and diuretic treatment in many scenarios provide further evidence of the involvement of several other contributing factors to the development of cardiogenic pulmonary edema. Several experimental and clinical studies have found that sympathetic overactivity with elevated plasma catecholamine concentrations may play an important role in the development of cardiovascular-associated pulmonary edema. Catecholamine-induced pulmonary injury may be one of the key mechanisms in acute cardiogenic pulmonary edema triggering proinflammatory cytokine overactivation, oxidative stress and myocardial injury. In the everyday treatment of acute heart failure, physicians should consider the possibility of other noncardiogenic mechanisms involved in the progression of acute pulmonary edema, particularly catecholamine overactivity, lymphatic drainage, inflammatory and oxidative stress, high surfactant protein. The classic, hemodynamic treatment approach in pulmonary edema with the coexistence of other contributing factors may not provide adequate clinical benefit during treatment.
Keywords: Pulmonary edema; acute heart failure; adrenoblocking therapy; alpha and beta adrenergic mechanism; capillary pressure; catecholamine; surfactant B protein.
AJCD Copyright © 2024.
Conflict of interest statement
None.
Figures
References
-
- Edoute Y, Roguin A, Behar D, Reisner SA. Prospective evaluation of pulmonary edema. Crit Care Med. 2000;28:330–335. - PubMed
-
- Hubble MW, Richards ME, Wilfong DA. Estimates of cost-effectiveness of prehospital continuous positive airway pressure in the management of acute pulmonary edema. Prehosp Emerg Care. 2008;12:277–285. - PubMed
-
- Dasta JF, McLaughlin TP, Mody SH, Piech CT. Daily cost of an intensive care unit day: the contribution of mechanical ventilation. Crit Care Med. 2005;33:1266–71. - PubMed
-
- Erdmann AJ 3rd, Vaughan TR Jr, Brigham KL, Woolverton WC, Staub NC. Effect of increased vascular pressure on lung fluid balance in unanesthetized sheep. Circ Res. 1975;37:271–84. - PubMed
-
- Arieff AI. Fatal postoperative pulmonary edema: pathogenesis and literature review. Chest. 1999;115:1371–1377. - PubMed
Publication types
LinkOut - more resources
Full Text Sources