

Cardiovascular outcomes of emergent vs elective transcatheter aortic valve replacement in severe aortic stenosis: regression matched meta-analysis
- PMID: 38764548
- PMCID: PMC11101960
- DOI: 10.62347/PORE5631
Cardiovascular outcomes of emergent vs elective transcatheter aortic valve replacement in severe aortic stenosis: regression matched meta-analysis
Abstract
Background: Transcatheter aortic valve replacement (TAVR) has been highly increased as the recommended option for patients with a high surgical risk. This study aims to commit a systematic review and meta-analysis to assess the outcomes in severe aortic stenosis patients following emergency transcatheter aortic valve replacement (emergent TAVR) compared to elective TAVR or eBAV followed by elective TAVR.
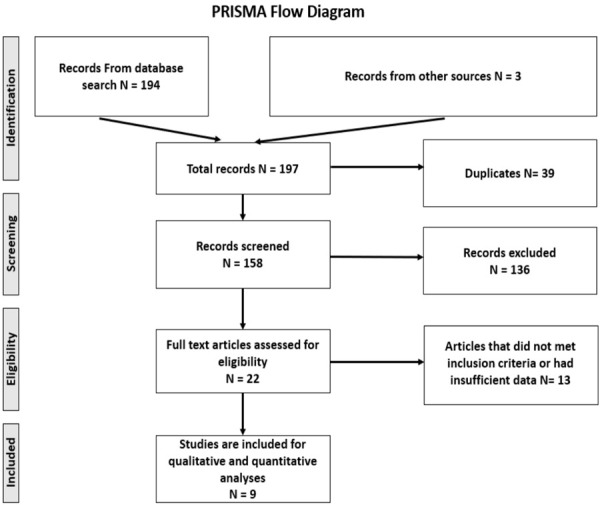
Methods: We conducted a systematic literature search of PubMed, Embase, Cochrane CENTRAL, CINAHL, Science Direct, and Google Scholar. We included nine studies in the latest analysis that reported the desired outcomes. Outcomes were classified into primary outcomes: 30-day all-cause mortality and 30-day readmission rate, and secondary outcomes, which were further divided into (a) peri-procedural outcomes, (b) vascular outcomes, and (c) renal outcomes. Statistical analysis was performed using Stata v.17 (College State, TX) software.
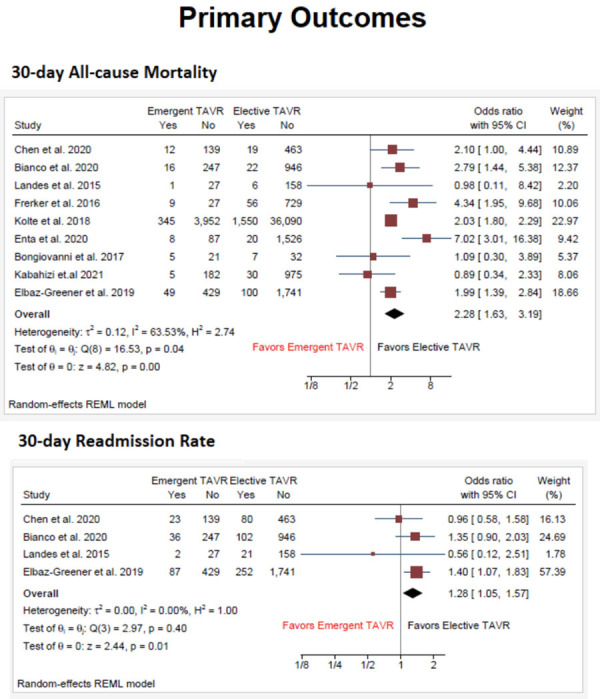
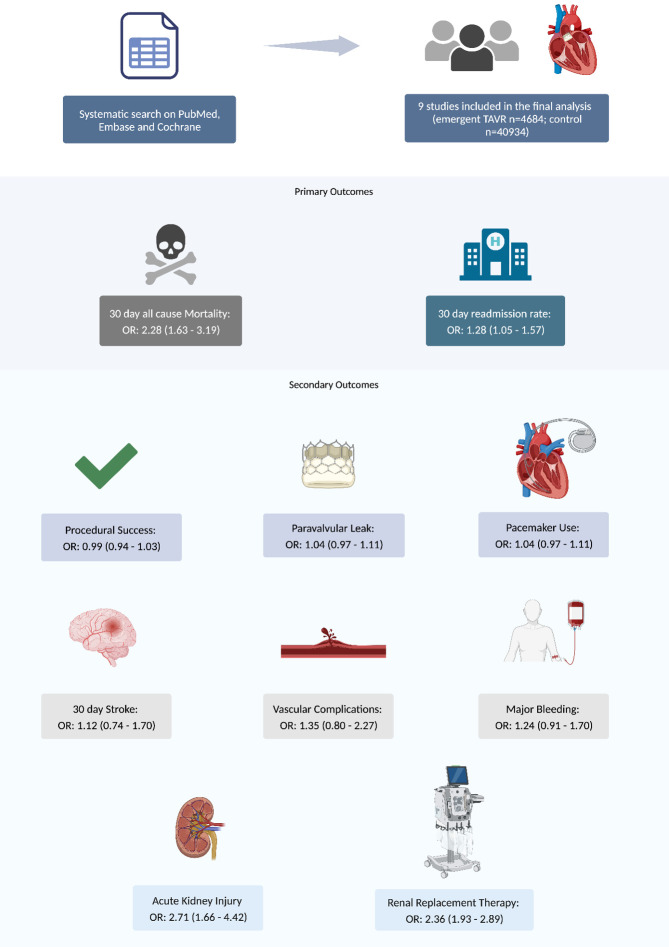
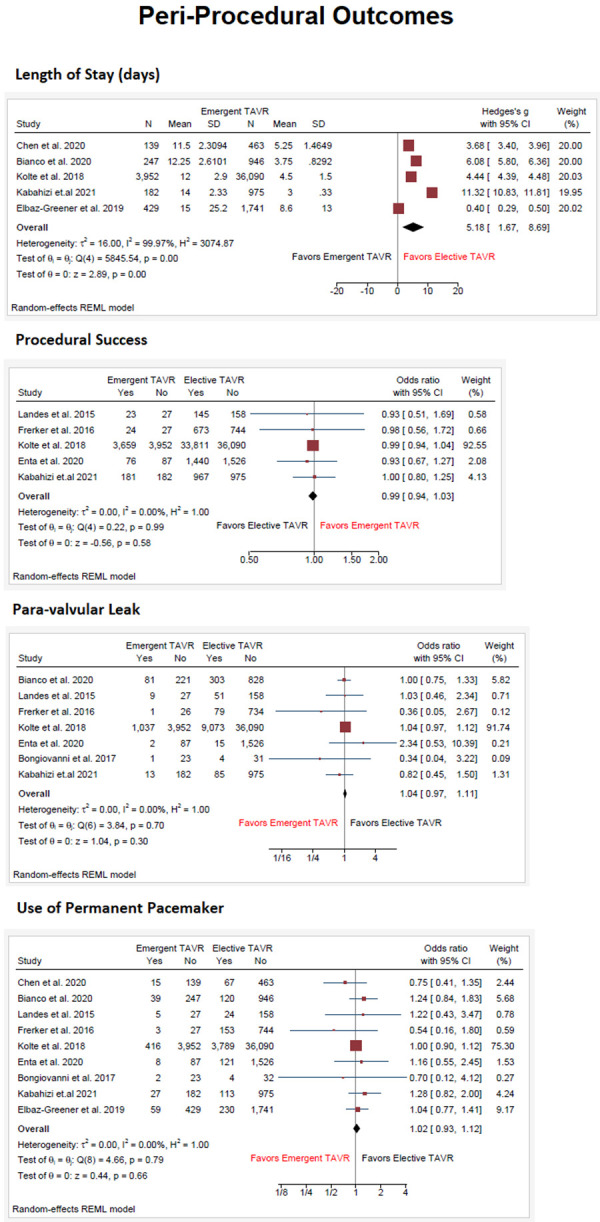
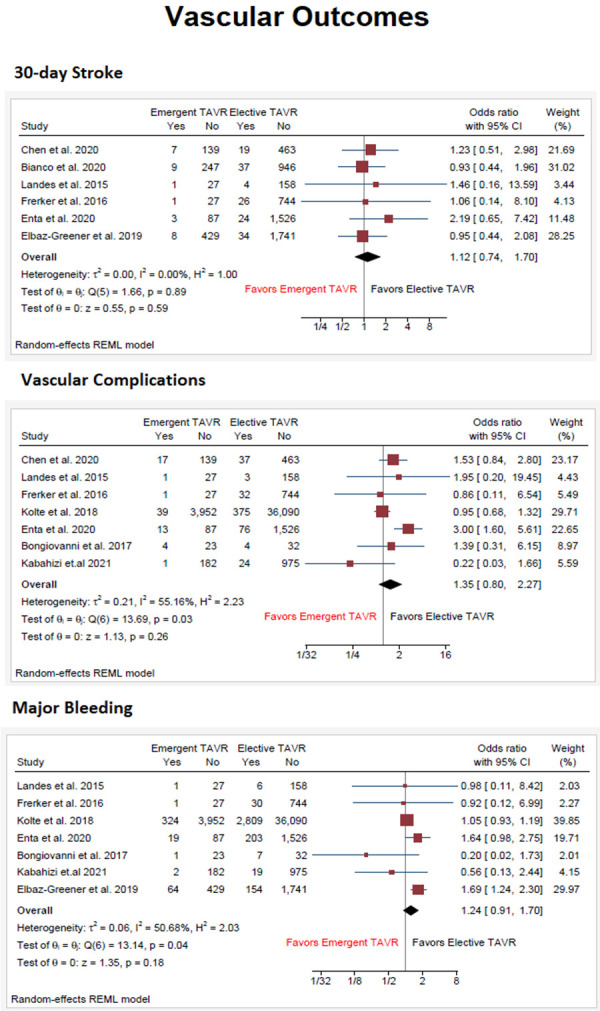
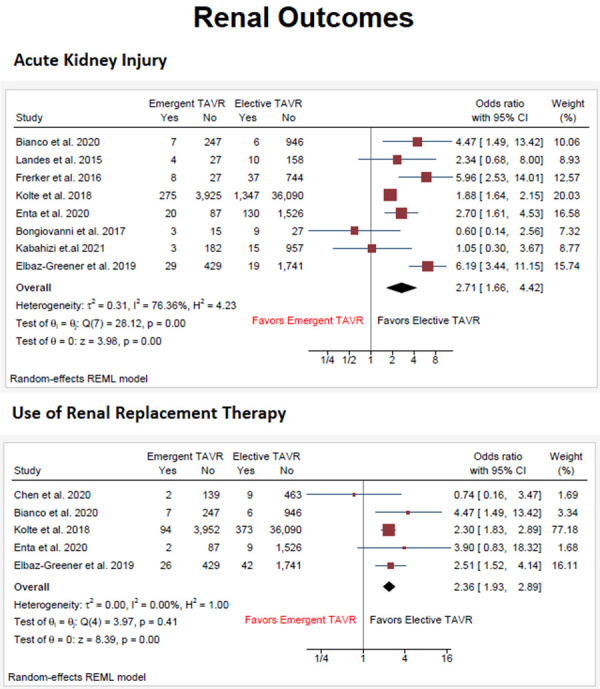
Results: A total of 44,731 patients with severe aortic stenosis were included (emergent TAVR n = 4502; control n = 40045). 30-day mortality was significantly higher in the emergent TAVR group (OR: 2.62; 95% CI = 1.76-3.92; P < 0.01). Regarding post-procedural outcomes, the length of stay was significantly higher in the emergent TAVR group (Hedges's g: +4.73 days; 95% CI = +3.35 to +6.11; P < 0.01). With respect to vascular outcomes, they were similar in both groups. Regarding renal outcomes, both acute kidney injury (OR: 2.52; 95% CI = 1.59-4.00; P < 0.01) and use of renal replacement therapy (OR: 2.33; 95% CI = 1.87-2.91; P < 0.01) were significantly higher in emergent TAVR group as compared to the control group.
Conclusion: Our study demonstrated that despite increased 30-day mortality and worse renal outcomes, the post-procedural outcomes were similar in emergent and elective TAVR groups. The increased mortality and worse renal outcomes are likely due to hemodynamic instability in the emergent group. The similarity of post-procedural outcomes is evidence of the safety of TAVR even in emergent settings.
Keywords: Emergent TAVR; aortic stenosis; elective TAVR.
AJCD Copyright © 2024.
Conflict of interest statement
None.
Figures
Similar articles
-
Outcomes Following Urgent/Emergent Transcatheter Aortic Valve Replacement: Insights From the STS/ACC TVT Registry.JACC Cardiovasc Interv. 2018 Jun 25;11(12):1175-1185. doi: 10.1016/j.jcin.2018.03.002. Epub 2018 Mar 11. JACC Cardiovasc Interv. 2018. PMID: 29929641
-
Outcomes of Adults with Severe Aortic Stenosis Undergoing Urgent or Emergent vs. Elective Transcatheter Aortic Valve Replacement Within an Integrated Health Care Delivery System.Struct Heart. 2023 Mar 21;7(4):100166. doi: 10.1016/j.shj.2023.100166. eCollection 2023 Jul. Struct Heart. 2023. PMID: 37520133 Free PMC article.
-
Valve-in-valve transcatheter aortic valve replacement versus redo surgical valve replacement for degenerated bioprosthetic aortic valve: An updated meta-analysis comparing midterm outcomes.Catheter Cardiovasc Interv. 2021 Jun 1;97(7):1481-1488. doi: 10.1002/ccd.29541. Epub 2021 Feb 13. Catheter Cardiovasc Interv. 2021. PMID: 33580743
-
Comparison of rehabilitation outcomes for transcatheter versus surgical aortic valve replacement as redo procedure in patients with previous cardiac surgery: Evidence based on 11 observational studies.Medicine (Baltimore). 2021 Nov 12;100(45):e27657. doi: 10.1097/MD.0000000000027657. Medicine (Baltimore). 2021. PMID: 34766568 Free PMC article.
-
[Comparison on the prognosis of severe aortic stenosis patients treated with transcatheter aortic valve replacement versus surgical aortic valve replacement: a systematic review and meta-analysis].Zhonghua Xin Xue Guan Bing Za Zhi. 2022 Sep 24;50(9):913-919. doi: 10.3760/cma.j.cn112148-20220211-00100. Zhonghua Xin Xue Guan Bing Za Zhi. 2022. PMID: 36096710 Chinese.
Cited by
-
Transcatheter Aortic Valve Implantation in Cardiogenic Shock: Current Evidence, Clinical Challenges, and Future Directions.J Clin Med. 2025 Jul 31;14(15):5398. doi: 10.3390/jcm14155398. J Clin Med. 2025. PMID: 40807025 Free PMC article. Review.
References
-
- Rawasia WF, Usman MS, Mujeeb FA, Zafar M, Khan SU, Alkhouli M. Transcatheter versus surgical aortic valve replacement in low-surgical-risk patients: a meta-analysis of randomized-controlled trials and propensity-matched studies. Cardiovasc Revasc Med. 2020;21:612–618. - PubMed
-
- Pujari SH, Agasthi P. Aortic Stenosis. In: StatPearls. Treasure Island (FL): StatPearls Publishing Copyright © 2024, StatPearls Publishing LLC.; 2024. - PubMed
-
- Saito T, Numata Y, Yamanaka Y. Mitral and aortic valve stenosis in alkaptonuria. Asian Cardiovasc Thorac Ann. 2017;25:239–240. - PubMed
-
- Maher ER, Young G, Smyth-Walsh B, Pugh S, Curtis JR. Aortic and mitral valve calcification in patients with end-stage renal disease. Lancet. 1987;2:875–877. - PubMed
-
- Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM 3rd, Thompson A, Toly C. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e72–e227. - PubMed
Publication types
LinkOut - more resources
Full Text Sources