

Case report: 'Atypical Richter transformation from CLL-type monoclonal B-cell lymphocytosis into Burkitt lymphoma in a treatment naïve patient'
- PMID: 38764580
- PMCID: PMC11099200
- DOI: 10.3389/fonc.2024.1296238
Case report: 'Atypical Richter transformation from CLL-type monoclonal B-cell lymphocytosis into Burkitt lymphoma in a treatment naïve patient'
Abstract
Background: Richter transformation refers to the progression of an initially slow-growing small lymphocytic lymphoma/chronic lymphocytic leukemia (SLL/CLL) into an aggressive lymphoma, typically diffuse large B-cell lymphoma (DLBCL) or Hodgkin lymphoma.
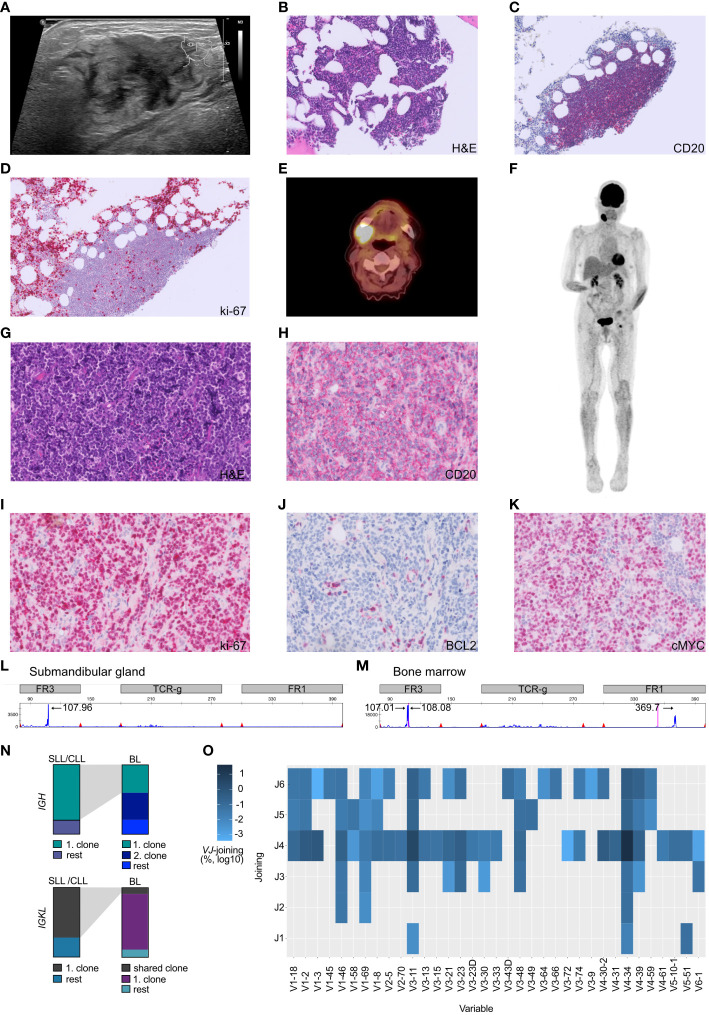
Case presentation: The patient presented with a rapid onset of localized cervical swelling, accompanied by monoclonal B-cell lymphocytosis displaying a CLL immunophenotype. The histopathological analysis identified a Burkitt lymphoma (BL) located in the submandibular gland and adjacent lymph node. The patient's bone marrow displayed a minor infiltration of monoclonal B-cells with a CLL immunophenotype (< 10%). Molecular analysis demonstrated the presence of the same monoclonal rearrangement in the framework region (FR3 region) of the immunoglobulin heavy chain (IGH) locus. High-throughput sequencing of the immunoglobulin heavy and light chains also confirmed the presence of the same rearrangement in SLL/CLL and in the Burkitt lymphoma sample, but also highlighted the presence of a second rearrangement in the Burkitt lymphoma cells, not shared with the SLL/CLL cells in the bone marrow. The patient was treated with DA-EPOCH-R, which lead to a complete metabolic response.
Conclusion: This report provides an exceptionally rare description of a CLL-type monoclonal B-cell lymphocytosis transforming into a very aggressive Burkitt lymphoma in a treatment naïve patient.
Keywords: Burkitt lymphoma; MBL; Richter transformation; SLL/CLL; state sequencing.
Copyright © 2024 Jauch, Alborelli, Reusser, Baschong, Rütsche, Bignucolo, Passweg, Dirnhofer and Krasniqi.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
Similar articles
-
Monoclonal B-cell lymphocytosis in the bone marrow: revisiting the criteria for chronic lymphocytic leukemia/small lymphocytic lymphoma.Hum Pathol. 2022 Jul;125:108-116. doi: 10.1016/j.humpath.2022.04.010. Epub 2022 Apr 25. Hum Pathol. 2022. PMID: 35472399
-
Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma With Secondary Acquisition of t(11;14)(q13;q32)/CCND1-IGH: A Rare Variant Of Richter Transformation to Mantle Cell Lymphoma.Clin Lymphoma Myeloma Leuk. 2022 May;22(5):e310-e313. doi: 10.1016/j.clml.2021.10.017. Epub 2021 Nov 3. Clin Lymphoma Myeloma Leuk. 2022. PMID: 34840090
-
PD-1 Expression in Chronic Lymphocytic Leukemia/Small Lymphocytic Lymphoma (CLL/SLL) and Large B-cell Richter Transformation (DLBCL-RT): A Characteristic Feature of DLBCL-RT and Potential Surrogate Marker for Clonal Relatedness.Am J Surg Pathol. 2018 Jul;42(7):843-854. doi: 10.1097/PAS.0000000000001077. Am J Surg Pathol. 2018. PMID: 29762141
-
Composite mantle cell lymphoma and chronic lymphocytic leukemia/small lymphocytic lymphoma: a clinicopathologic and molecular study.Hum Pathol. 2013 Jan;44(1):110-21. doi: 10.1016/j.humpath.2012.04.022. Epub 2012 Aug 31. Hum Pathol. 2013. PMID: 22944294 Free PMC article. Review.
-
Richter syndrome in chronic lymphocytic leukemia: updates on biology, clinical features and therapy.Leuk Lymphoma. 2015 Jul;56(7):1949-58. doi: 10.3109/10428194.2014.979411. Epub 2015 Jan 21. Leuk Lymphoma. 2015. PMID: 25356923 Review.
References
-
- Swerdlow S, Campo E, Harris N, Jaffe E, Pileri S, Stein H, et al. . WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues, 4th. (2017). LYON, France: WHO. Available at: https://www.iarc.who.int/news-events/who-classification-of-tumours-of-ha....
-
- Lortholary P, Boiron M, Ripault P, Levy JP, Manus A, Bernard J. Leucemie Lymphoide Chronique secondairement associée à une Réticulopathie Maligne, Syndrome de Richter. Nouv Rev Fr Hematol. (1964) 4:621–44. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Miscellaneous