

Development and validation of a novel nomogram model for identifying risk of prolonged length of stay among patients receiving free vascularized flap reconstruction of head and neck cancer
- PMID: 38764582
- PMCID: PMC11099871
- DOI: 10.3389/fonc.2024.1345766
Development and validation of a novel nomogram model for identifying risk of prolonged length of stay among patients receiving free vascularized flap reconstruction of head and neck cancer
Abstract
Background: The aim of the present study was to build and internally validate a nomogram model for predicting prolonged length of stay (PLOS) among patients receiving free vascularized flap reconstruction of head and neck cancer (HNC).
Methods: A retrospective clinical study was performed at a single center, examining patients receiving free vascularized flap reconstruction of HNC from January 2011 to January 2019. The variables were obtained from the electronic information system. The primary outcome measure was PLOS. Univariate and multivariate analyses were used to find risk factors for predicting PLOS. A model was then built according to multivariate results. Internal validation was implemented via 1000 bootstrap samples.
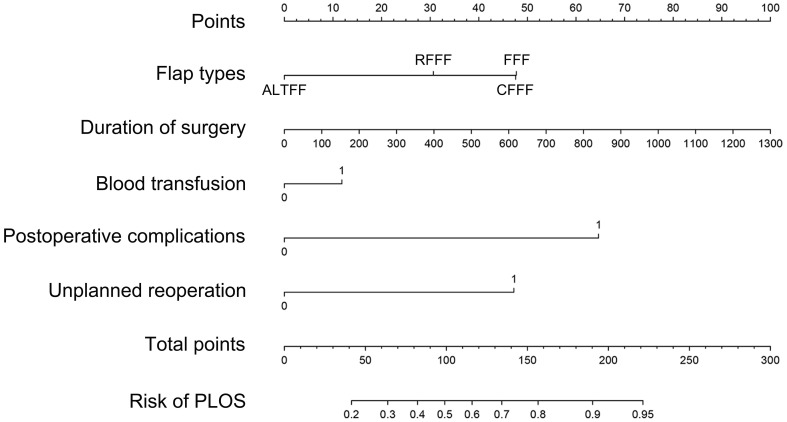
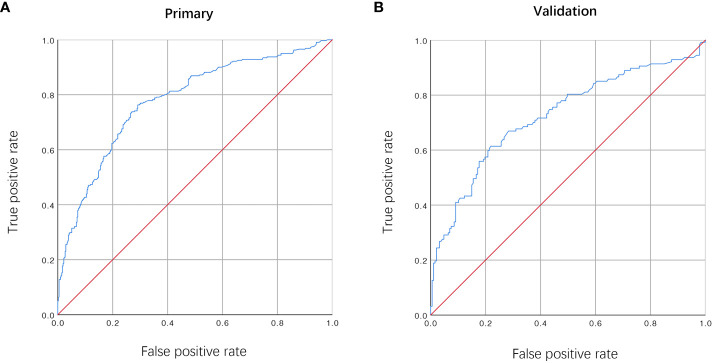
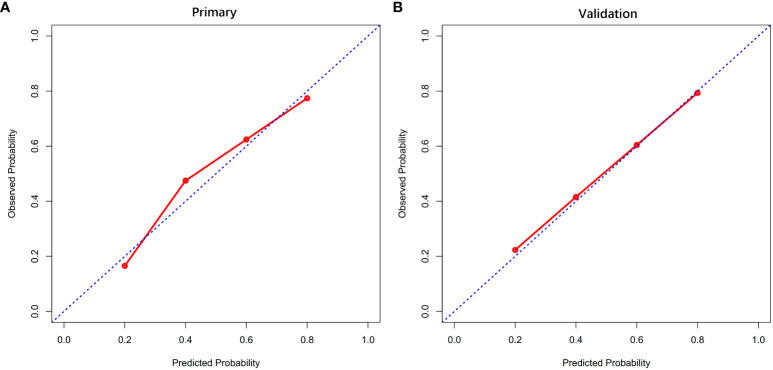
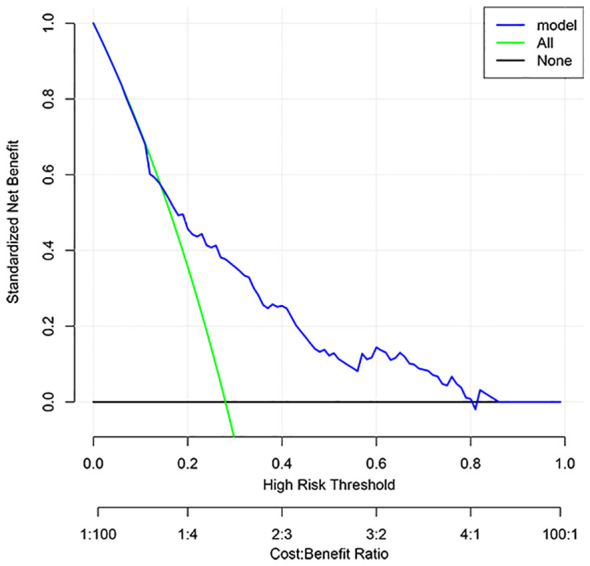
Results: The study included 1047 patients, and the median length of stay (LOS) was 13.00 (11.00, 16.00) days. Multivariate analysis showed that flap types ((radial forearm free flap (odds ratio [OR] = 2.238; 95% CI, 1.403-3.569; P = 0.001), free fibula flap (OR = 3.319; 95% CI, 2.019-4.882; P < 0.001)), duration of surgery (OR = 1.002; 95% CI, 1.001-1.003; P = 0.004), postoperative complications (OR = 0.205; 95% CI, 0.129-0.325; P = P < 0.001) and unplanned reoperation (OR = 0.303; 95% CI, 0.140-0.653; P = 0.002) were associated with PLOS. In addition to these variables, blood transfusion was comprised in the model. The AUC of the model was 0.78 (95% CI, 0.711-0.849) and 0.725 (95% CI, 0.605-0.845) in the primary and internal validation cohorts, respectively. The DCA revealed the clinical utility of the current model when making intervention decisions within the PLOS possibility threshold range of 0.2-0.8.
Conclusions: Our study developed a nomogram that exhibits a commendable level of accuracy, thereby aiding clinicians in assessing the risk of PLOS among patients receiving free vascularized flap reconstruction for HNC.
Keywords: free vascularized flap; head and neck cancer; length of hospital stay; nomogram; reconstruction.
Copyright © 2024 Wang, Lin, Wu, Fu, Liu and Cao.
Conflict of interest statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Figures
References
-
- Tapia B, Garrido E, Cebrian JL, Del Castillo JL, Gonzalez J, Losantos I, et al. . Impact of goal directed therapy in head and neck oncological surgery with microsurgical reconstruction: Free flap viability and complications. Cancers (Basel). (2021) 13(7):1545. doi: 10.3390/cancers13071545 - DOI - PMC - PubMed
-
- Girod A, Brancati A, Mosseri V, Kriegel I, Jouffroy T, Rodriguez J. Study of the length of hospital stay for free flap reconstruction of oral and pharyngeal cancer in the context of the new French casemix-based funding. Oral Oncol. (2010) 46:190–4. doi: 10.1016/j.oraloncology.2009.12.002 - DOI - PubMed
LinkOut - more resources
Full Text Sources