

Association between changes in cardiovascular health and the risk of multimorbidity: community-based cohort studies in the UK and Finland
- PMID: 38764806
- PMCID: PMC11098950
- DOI: 10.1016/j.lanepe.2024.100922
Association between changes in cardiovascular health and the risk of multimorbidity: community-based cohort studies in the UK and Finland
Abstract
Background: Better cardiovascular health is associated with lower risk of various chronic diseases, but its association with multimorbidity is poorly understood. We aimed to examine whether change in cardiovascular health is associated with multimorbidity risk.
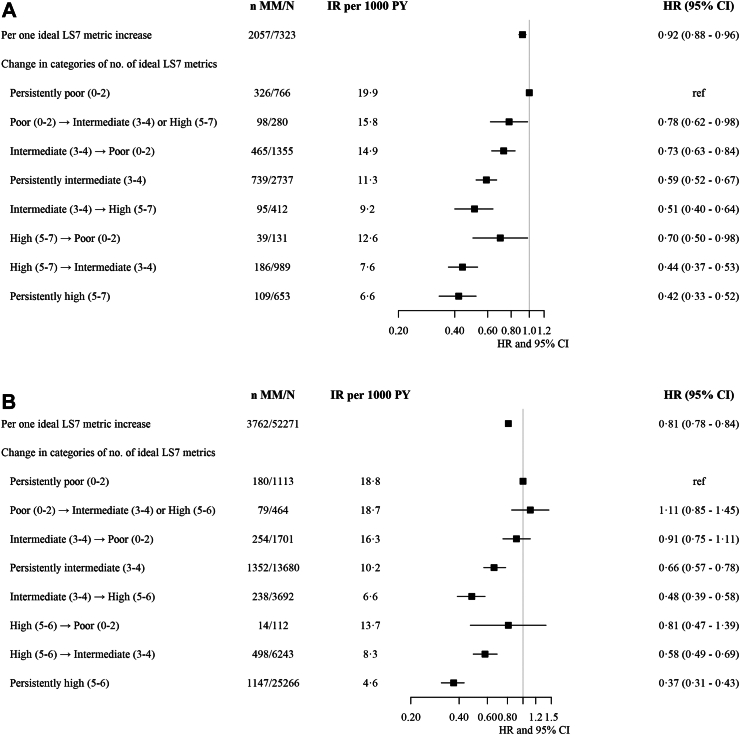
Methods: The primary analysis was conducted in the Whitehall II multiwave prospective cohort study (UK) and the validation analysis in the Finnish Public Sector cohort study (Finland). Change in cardiovascular health was assessed using the American Heart Association Life's Simple 7 (LS7) and Life's Essential 8 (LE8) at baseline and re-assessments, using objective measures in Whitehall II and self-reports and pharmacy claims in the Finnish Public Sector cohort study, respectively. Multimorbidity was defined as the presence of two or more of 12 chronic diseases during follow-up. We estimated hazard ratios (HR) and 95% confidence intervals (CI) using Cox's proportional hazard models with age as time scale, adjusting for sex, education, occupation, marital status, and ethnicity.
Findings: In the primary analysis among 9715 participants, mean age was 44.8 (standard deviation 6.0) years and 67.6% participants were men at baseline. During the median follow-up of 31.4 (interquartile range 26.8-32.3) years, 2751 participants developed multimorbidity. The hazard of multimorbidity decreased by 8% (HR 0.92, 95% CI 0.88-0.96) per ideal LS7 metric increment over 5 years and by 14% (HR 0.86, 95% CI 0.80-0.93) per ten points increase in LE8 score over 10 years. These findings were replicated in the validation analysis among 75,377 participants in terms of 4-year change in cardiovascular health.
Interpretation: Improvement in cardiovascular health was associated with lower multimorbidity risk in two community-based cohort studies. Interventions improving cardiovascular health of the community may contribute to multimorbidity prevention.
Funding: None.
Keywords: Cardiovascular health; Chronic diseases; Cohort study; Multimorbidity; Prevention.
© 2024 The Author(s).
Conflict of interest statement
The authors declare no competing interests.
Figures

References
-
- Lloyd-Jones D.M., Hong Y., Labarthe D., et al. Defining and setting national goals for cardiovascular health promotion and disease reduction: the American Heart Association's strategic Impact Goal through 2020 and beyond. Circulation. 2010;121:586–613. - PubMed
-
- Uijl A., Koudstaal S., Vaartjes I., et al. Risk for heart failure: the opportunity for prevention with the American heart association's life's simple 7. JACC Heart Fail. 2019;7(8):637–647. - PubMed
LinkOut - more resources
Full Text Sources
