

Hyperkalaemia in bleeding trauma patients: A potential marker of disease severity - A retrospective cohort study
- PMID: 38765110
- PMCID: PMC11101751
- DOI: 10.1016/j.heliyon.2024.e30037
Hyperkalaemia in bleeding trauma patients: A potential marker of disease severity - A retrospective cohort study
Abstract
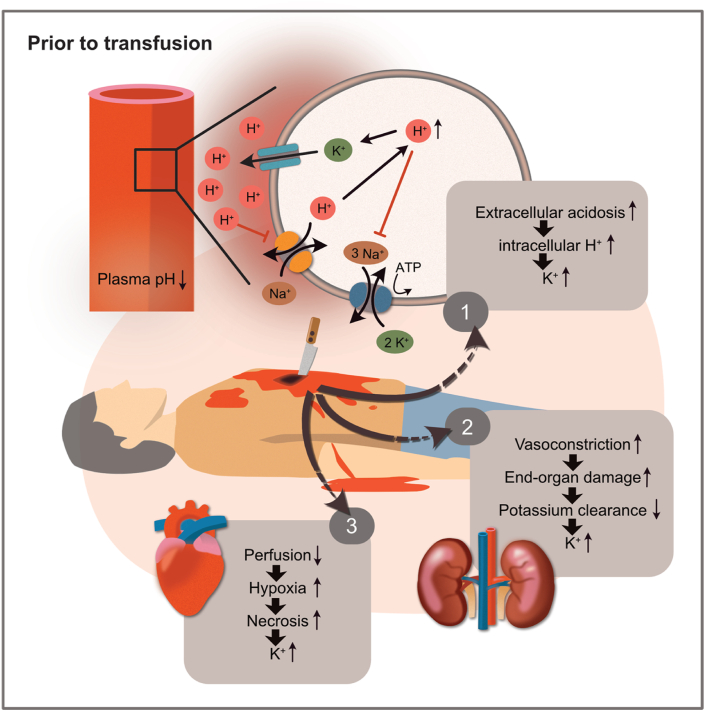
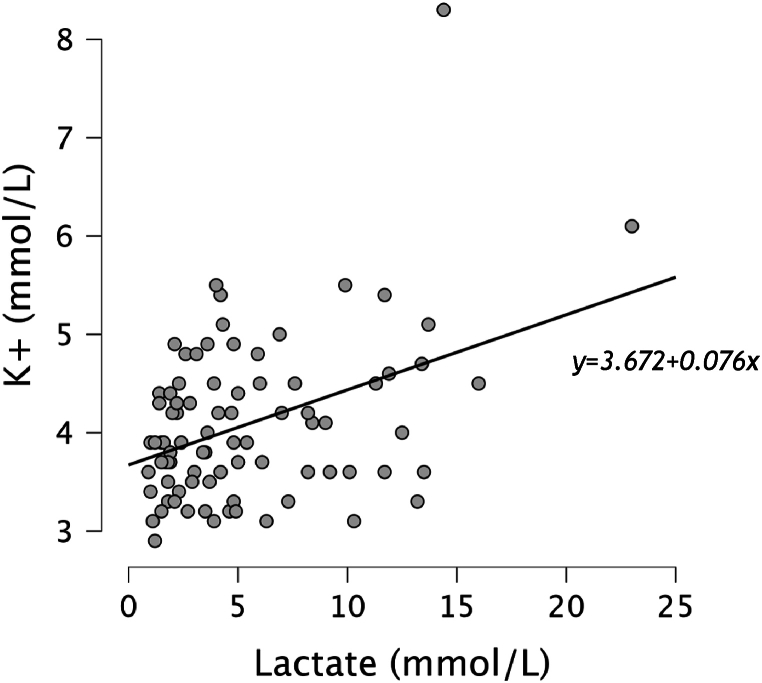
Background: Hyperkalaemia is a common electrolyte abnormality seen in critically ill patients. In haemorrhagic shock, it may contribute to cardiac arrest and has been identified as a potential marker for tissue hypoxia. However, the significance of its role in haemorrhagic shock and its contribution to mortality remains unclear. This study aimed to examine the potential underlying pathophysiology and evaluate the incidence and characteristics of patients with hyperkalaemia on hospital arrival in bleeding trauma patients before transfusions and its mortality.
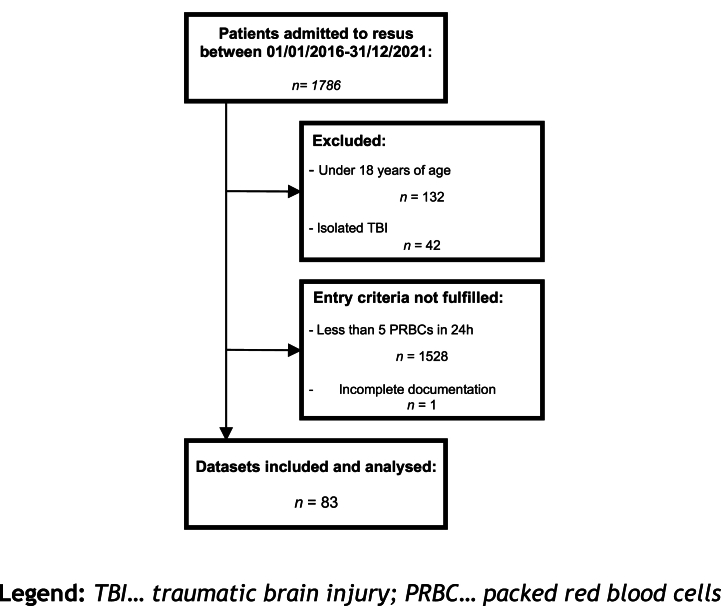
Methods: A retrospective cohort study was conducted on adult patients with traumatic bleeding admitted to a European Major Trauma Centre between January 2016 and December 2021. Patients were classified according to their serum potassium levels on arrival, and relevant clinical parameters between non-hyperkalaemic and hyperkalaemic patients were compared.
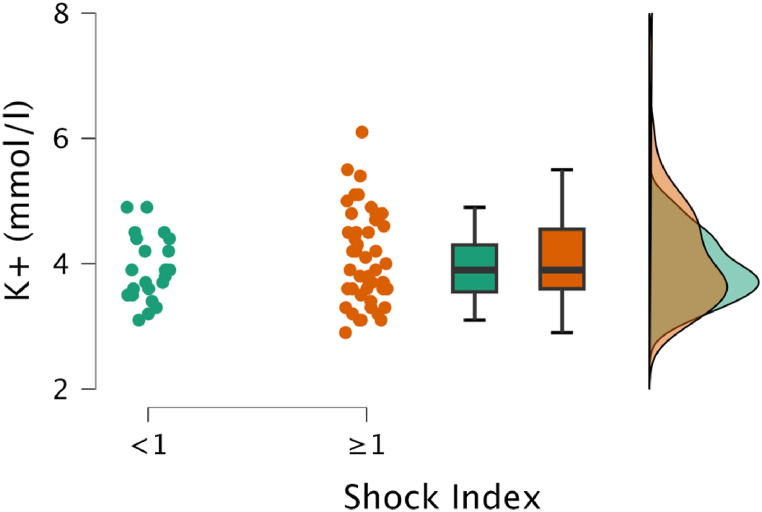
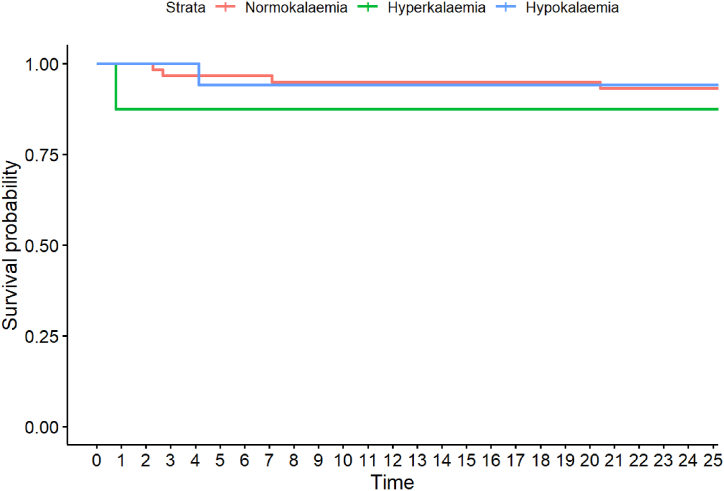
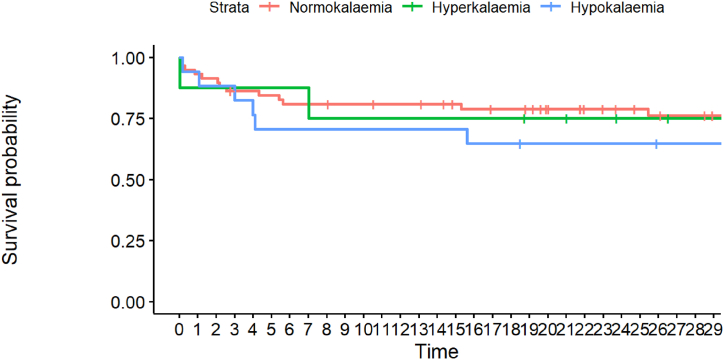
Results: Among the 83 patients in this study, 8 (9.6 %) presented with hyperkalaemia on arrival. The median shock index showed a higher tendency in the hyperkalaemic group. Hyperkalaemia was found to be more common among younger patients who sustained penetrating trauma. Mortality rates were higher in the hyperkalaemic group, but the difference was not statistically significant.
Conclusion: Our results suggest that hyperkalaemia occurs frequently in bleeding trauma patients on hospital arrival pre-transfusions, indicating a more severe illness. Our findings provide insights into the pathophysiology and characteristics of hyperkalaemia in bleeding trauma patients. Further studies are required to investigate the mechanisms by which hyperkalaemia contributes to mortality in haemorrhagic shock patients.
Keywords: Haemorrhage; Ischemia; Multiple trauma; Potassium; Shock.
© 2024 The Authors.
Conflict of interest statement
ME, MR, ME2, AP, PZ, HB and PZ1 report no conflicts of interest.
Figures
References
-
- Evans J.A., Van Wessem K.J.P., McDougall D., Lee K.A., Lyons T., Balogh Z.J. Epidemiology of traumatic deaths: comprehensive population-based assessment. World J. Surg. 2010;34(1):158–163. - PubMed
-
- Jansen J.O., Hudson J., Cochran C., Maclennan G., Lendrum R., Sadek S., et al. Emergency department resuscitative endovascular balloon occlusion of the aorta in trauma patients with exsanguinating hemorrhage: the UK-REBOA randomized clinical trial. JAMA. 2023;330(19) https://pubmed.ncbi.nlm.nih.gov/37824132/ - PMC - PubMed
-
- Braverman M.A., Smith A., Pokorny D., Axtman B., Shahan C.P., Barry L., et al. Prehospital whole blood reduces early mortality in patients with hemorrhagic shock. Transfusion (Paris) 2021;61(S1) https://onlinelibrary.wiley.com/doi/full/10.1111/trf.16528 - DOI - PubMed
-
- Castellini G., Gianola S., Biffi A., Porcu G., Fabbri A., Ruggieri M.P., et al. Resuscitative endovascular balloon occlusion of the aorta (REBOA) in patients with major trauma and uncontrolled haemorrhagic shock: a systematic review with meta-analysis. World J. Emerg. Surg. 2021;16(1):1–12. https://link.springer.com/articles/10.1186/s13017-021-00386-9 - DOI - PMC - PubMed
-
- Cannon J.W., Shock Hemorrhagic, Longo D.L., editors. vol. 378. 2018. pp. 370–379. (New England Journal of Medicine).
LinkOut - more resources
Full Text Sources
