

Prospective Study on Individualized Dose Adjustment of Tolvaptan Based on Urinary Osmolality in Patients With ADPKD
- PMID: 38765583
- PMCID: PMC11101827
- DOI: 10.1016/j.ekir.2024.01.020
Prospective Study on Individualized Dose Adjustment of Tolvaptan Based on Urinary Osmolality in Patients With ADPKD
Abstract
Introduction: Tolvaptan has been shown to reduce renal volume and delay disease progression in autosomal-dominant polycystic kidney disease (ADPKD). However, no biomarkers are currently available to guide dose adjustment. We aimed to explore the possibility of individualized tolvaptan dose adjustments based on cut-off values for urinary osmolality (OsmU).
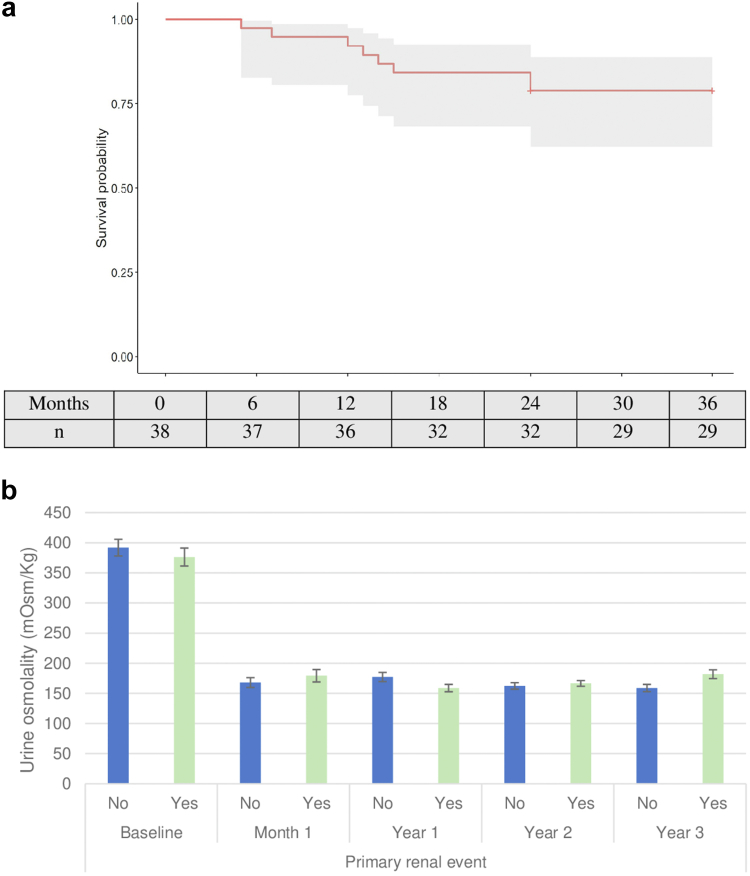
Methods: This prospective cohort study included patients with ADPKD, with rapid disease progression. Tolvaptan treatment was initiated at a dose of 45/15 mg and increased based on OsmU, with a limit set at 200 mOsm/kg. Primary renal events (25% decrease in estimated glomerular filtration rate [eGFR] during treatment), within-patient eGFR slope, and side effects were monitored during the 3-year follow-up.
Results: Forty patients participated in the study. OsmU remained below 200 mOsm/kg throughout the study period, and most patients required the minimum tolvaptan dose (mean dose, 64 [±10] mg), with a low discontinuation rate (5%). The mean annual decline in eGFR was -3.05 (±2.41) ml/min per 1.73 m2 during tolvaptan treatment, compared to the period preceding treatment, corresponding to a reduction in eGFR decline of more than 50%. Primary renal events occurred in 20% of patients (mean time to onset, 31 months; 95% confidence interval [CI] = 28-34).
Conclusion: Individualized tolvaptan dose adjustment based on OsmU in patients with ADPKD and rapid disease progression provided benefits in terms of reducing eGFR decline, compared with reference studies, and displayed lower dropout rates and fewer side effects. Further studies are required to confirm optimal strategies for the use of OsmU for tolvaptan dose adjustment in patients with ADPKD.
Keywords: autosomal-dominant polycystic kidney disease; estimated glomerular filtration rate; tolvaptan; urinary osmolality.
© 2024 International Society of Nephrology. Published by Elsevier Inc.
Figures




Similar articles
-
Tolvaptan and Autosomal Dominant Polycystic Kidney Disease Progression in Individuals Aged 18-35 Years: A Pooled Database Analysis.Kidney Med. 2024 Nov 14;7(1):100935. doi: 10.1016/j.xkme.2024.100935. eCollection 2025 Jan. Kidney Med. 2024. PMID: 39810815 Free PMC article.
-
Low-dose tolvaptan to control disease progression in Chinese patients with autosomal dominant polycystic kidney disease: a retrospective cohort study.Transl Androl Urol. 2024 Oct 31;13(10):2307-2321. doi: 10.21037/tau-24-448. Epub 2024 Oct 28. Transl Androl Urol. 2024. PMID: 39507867 Free PMC article.
-
Effectiveness of Tolvaptan for Autosomal Dominant Polycystic Kidney Disease in US Clinical Practice With Comparison to Historical Control Data.Kidney Med. 2025 Feb 27;7(5):100988. doi: 10.1016/j.xkme.2025.100988. eCollection 2025 May. Kidney Med. 2025. PMID: 40242785 Free PMC article.
-
Clinical Utility and Tolerability of Tolvaptan in the Treatment of Autosomal Dominant Polycystic Kidney Disease (ADPKD).Drug Healthc Patient Saf. 2022 Sep 8;14:147-159. doi: 10.2147/DHPS.S338050. eCollection 2022. Drug Healthc Patient Saf. 2022. PMID: 36105663 Free PMC article. Review.
-
Assessing Risk of Rapid Progression in Autosomal Dominant Polycystic Kidney Disease and Special Considerations for Disease-Modifying Therapy.Am J Kidney Dis. 2021 Aug;78(2):282-292. doi: 10.1053/j.ajkd.2020.12.020. Epub 2021 Mar 8. Am J Kidney Dis. 2021. PMID: 33705818 Review.
Cited by
-
Cost-Minimization Analysis of Tolvaptan Treatment for ADPKD in Southern Spain.Kidney Int Rep. 2024 Oct 26;10(1):265-266. doi: 10.1016/j.ekir.2024.10.024. eCollection 2025 Jan. Kidney Int Rep. 2024. PMID: 39810782 Free PMC article. No abstract available.
-
What is the Appropriate Dose of Tolvaptan in ADPKD?Kidney Int Rep. 2024 Feb 1;9(4):737-739. doi: 10.1016/j.ekir.2024.01.049. eCollection 2024 Apr. Kidney Int Rep. 2024. PMID: 38765581 Free PMC article. No abstract available.
-
Response to the Letter to the Editor Entitled "Refining Tolvaptan Dosing in ADPKD: The Role of Urinary Biomarkers in Enhancing Outcomes".Kidney Int Rep. 2025 May 28;10(8):2880. doi: 10.1016/j.ekir.2025.05.040. eCollection 2025 Aug. Kidney Int Rep. 2025. PMID: 40814628 Free PMC article. No abstract available.
-
A Primer for Utilizing Deep Learning and Abdominal MRI Imaging Features to Monitor Autosomal Dominant Polycystic Kidney Disease Progression.Biomedicines. 2024 May 20;12(5):1133. doi: 10.3390/biomedicines12051133. Biomedicines. 2024. PMID: 38791095 Free PMC article. Review.
-
Prospective Study on Individualized Dose Adjustment of Tolvaptan Based on Urinary Osmolality in Patients With ADPKD.Kidney Int Rep. 2024 Nov 12;10(1):271. doi: 10.1016/j.ekir.2024.10.042. eCollection 2025 Jan. Kidney Int Rep. 2024. PMID: 39810775 Free PMC article. No abstract available.
References
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
